Pesquisa disponível em PDF. Clique aqui e faça o download do arquivo.
Índice
Objetivos e critérios de inclusão: 3
Anexo 1: Tabela de Artigos. 10
Artigos sobre Osteoartrite: 11
Análise de Pressão Plantar: 13
Equilíbrio e instabilidade: 14
Referências Bibliográficas: 17
Órteses plantares e palmilhas ortopédicas na prática clínica: uma revisão da literatura
Taddei UT; Case TA, Santos CV.
Resumo:
Objetivos: Coletar dados sobre a utilização de órteses plantares na literatura científica e descrever os benefícios encontrados no tratamento de diferentes moléstias.
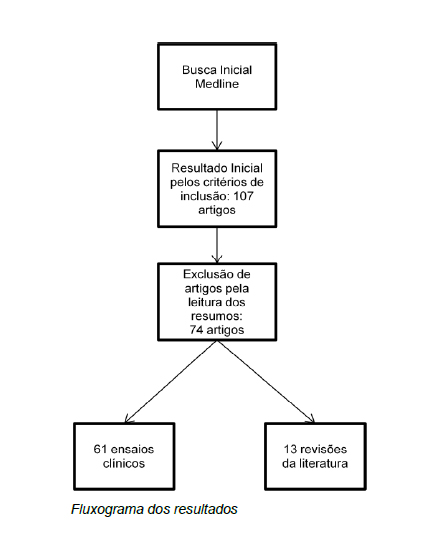
Métodos: Revisão da literatura segundo o “Center of Reviews and Dissemination guidance for undertaking reviews in health care” na base de dados Medline.
Resultados: Foram triados 74 artigos, 61 do tipo ensaio clínico e 13 revisões da literatura.
Conclusão: O uso de órteses plantares podem oferecer diversos benefícios como tratamento complementar nas mais diferentes áreas da saúde. Os mecanismos de ação pelos quais se justifica o resultado das órteses são de alteração biomecânica e postural, alteração e distribuição da pressão plantar, amortecimento de impactos por materiais macios e estimulação nervosa periférica. O tipo de órtese utilizada está relacionado à etiologia da moléstia a ser tratada, assim como o sucesso na utilização relaciona-se a escolha correta da órtese plantar. Enquanto se encontra um grande número de artigos na literatura sobre o uso de órteses plantares em casos de osteoartrite, pés diabéticos e fratura por estresse, faltam estudos relacionados à patologias mais comuns na prática clinica como neuroma de Morton e fascite plantar.
Palavras-Chave: Aparelhos Ortopédicos, Deformidades do Pé, Doenças do Pé, Órteses do Pé, Pé.
Introdução:
A utilização de órteses plantares como palmilhas e calçados especiais já é bem difundida na prática clinica ortopédica. São comumente usadas como tratamento conservador para a maioria dos problemas dos pés como fascite plantar, neuroma de Morton e até simples queixas de dores nos pés (Scheiber 2011, Caselli 1997, Benvenuti 1994).
São divididas basicamente em pré-fabricadas ou customizadas. As primeiras geralmente se baseiam em fornecer apoio para o arco longitudinal medial (ALM) ou conforto e amortecimento através de materiais que absorvem impactos. Já as customizadas possibilitam uma vasta gama de correções e adaptações a diferentes variações anatômicas, doenças estruturais ou funcionais.
Os materiais das quais são fabricadas variam de plásticos, espumas, borrachas, cortiça e não raramente são confeccionadas com mais de um material dependendo dos objetivos(Caseli 1997, Withnall 2006, Van Geffen 2007).
Figura 1: Palmilhas em EVA e Poron.
Sua prescrição tem como tentativa alterar a área de contato dos pés, alterar as pressões plantares ou mudar a biomecânica da postura e da marcha. Alguns estudos encontraram ainda diferenças na atividade muscular dos membros inferiores com o uso de palmilhas ortopédicas, relacionando essa diferença ao aumento da informação aferente de receptores cutâneos (Oishi 2011, Jahss 1981).
Um grande número de artigos na literatura compara os resultados do uso de diferentes tipos de palmilhas ortopédicas a outros métodos de tratamento para uma gama de doenças e sintomas. Em sua maioria, estes estudos utilizam como parâmetro de acompanhamento questionários para patologias específicas ou métodos de coleta antropométrica como baropodometria, plataformas de força e cinemetria.
Os objetivos e metodologias são os mais variados, embora as perguntas sejam sempre as mesmas: essas órteses funcionam? E, se funcionam como agem?
Este estudo tem por objetivo relatar as diferentes utilizações de palmilhas e outras órteses, descrever os tipos de órteses utilizadas e reportar a eficácia dessas formas de tratamento informadas em ensaios clínicos e revisões da literatura utilizando a base de dados MEDLINE.
Objetivos e critérios de inclusão:
O objetivo desta revisão é qualificar e quantificar os distúrbios em que se utilizam órteses plantares como forma terapêutica, descrever as órteses utilizadas em cada caso, o princípio no qual se baseiam e reportar a eficácia em cada caso.
Serão incluídos ensaios clínicos e revisões da literatura que se refiram a palmilhas e órteses plantares como forma terapêutica, prevenção, controle ou reabilitação de quaisquer doenças, publicados até 31/12/2012 nas línguas Inglesa, Portuguesa, Espanhola ou Francesa.
Metodologia:
Uma revisão da literatura foi realizada com base no “Center of Reviews and Dissemination guidance for undertaking reviews in health care”.
O time revisor contou com dois fisioterapeutas com experiência na prescrição e produção de órteses, um revisor estatístico com experiência de trabalho com pesquisas em saúde e um médico ortopedista especialista em distúrbios dos pés como revisor final.
Inicialmente, foi realizada uma busca na “Cochrane Database of Systematic Reviews” (CDSR) e no “National Institute for Health and Clinical Excellence” (NICE) com o objetivo de determinar se uma nova revisão é realmente necessária, no entanto nenhuma revisão com objetivos similares foi encontrada.
A busca por artigos científicos foi realizada na base de dados MEDLINE. Foi conduzida utilizando palavras-chave e descritores em ciências da saúde encontrados na Biblioteca virtual em saúde (BVS) e “Medical Subject Headings”, combinadas pelos operadores Booleanos (“AND”, “OR” e “NOT”).
Do número total de artigos, foram excluídos os que se repetissem em buscas diferentes, e os demais foram triados e só foram selecionados caso contivessem no título ou resumo os termos “insole”, “foot orthosis”, “arch pads”, “arch support”, “pedorthics” ou “footwear”.
Em seguida, dois fisioterapeutas realizaram a leitura dos resumos e excluíram estudos que não utilizassem palmilhas e órteses como forma de tratamento ou prevenção de alguma doença (como por exemplo, para coleta de dados antropométricos via palmilhas de baropodometria).
Foram incluídos no total 74 artigos sendo 13 revisões da literatura e 61 ensaios clínicos.
Resultados:
Os artigos triados estão apresentados no Anexo 1 que inclui o nome do autor e ano de publicação, tipo de estudo, o tema do estudo, a intervenção, o tipo de medida e os resultados de forma resumida.
Metatarsalgia primária:
Metatarsalgia é a dor ao redor da cabeça dos metatarsos ou nas articulações metatarso-falangeanas e nos tecidos moles adjacentes. Geralmente é relacionada a altos valores de pressão plantar e seu tratamento visa justamente a redistribuição pressórica no ante-pé. As formas mais usuais são através de orteses plantares, na forma de pilotos metatarsais, rockerbar (alteração em mataborrão no calçado), palmilhas planas para absorção de impactos e palmilhas customizadas (Postema 1998).
Postema et al. Pesquisou os efeitos de palmilhas customizadas, pré-fabricadas e rockerbar shoes com quatro combinações (palmilhas customizadas com e sem uso de rockerbar e palmilhas pré-fabricadas com e sem rockerbar) no tratamento da metatarsalgia primária em 42 sujeitos num ensaio clinico randomizado e duplo cego (Postema1998).
A coleta de dados foi realizada durante a marcha através de plataformas de pressão (EMED-SF pressure plataform) e o sistema Pedar (Mikro-EMED) e um questionário para avaliação da dor.
Foi encontrado que palmilhas customizadas e o uso de rockerbar resultam em redistribuição da pressão no antepé estatisticamente significante sem mostrar interação no uso simultâneo dos métodos.
Também foi relatada a preferência dos sujeitos pelas palmilhas customizadas, que mostraram melhora significativa nos níveis de dor.
Neuroma de Morton:
A primeira descrição da associação de neuroma e dores nos pés foi feita por Civinni (1835) e Durlacher (1845) e foi descrita mais tarde por Dudley Morton como uma dor metatarso-falangeana. Trata-se de uma fibrose perineural possivelmente causada pelo encarceramento dos nervos interdigitais dos pés, de diagnóstico primariamente baseado em achados clínicos, ultrassonografia e ressonância magnética (Spina 2002).
É mais prevalente em mulheres afetando mais frequentemente o terceiro espaço intermetatarsal.
Schreiber e colaboradores (2011) investigaram a literatura pelo melhor tratamento para neuroma de Morton e reportou que somente um ensaio clinico não controlado propunha um protocolo que incluía educação do paciente, mudança do tipo de calçado e palmilha, uso de corticoesteroides e, por fim, cirurgia. Embora possam ser encontrados relatos do uso de escleroterapia, a evidência cientifica se mostrou insuficiente.
Osteoartrite de Joelhos:
A Osteoartrite de joelho (OAJ) é um dos distúrbios mais comuns, afetando aproximadamente 6% dos adultos acima de 30 anos e sendo responsável por um maior número de incapacidades que qualquer outra doença. A OAJ geralmente compromete somente um dos compartimentos e a ocorrência medial é dez vezes maior que a lateral (Toda 2004).
O tratamento inicial é conservativo e consiste na orientação do paciente, redução de peso, fisioterapia e medicação (Van Raaij 2010).
Foram encontrados 22 estudos com órteses plantares em osteoartrite. Destes, 14 investigaram a adição de cunhas laterais no tratamento da OAJ medial.
Shimada (2006) analisou o índice de Kellgren-Lawrence em 42 sujeitos de dois grupos, OA e controle, reportou a diminuição do momento adutor nos joelhos e concluiu que é recomendável o uso de palmilhas com cunha lateral em pacientes em estágios pouco avançados de OAJ.
Pham (2004) não encontrou diferenças entre os grupos estudados (Cunha lateral contra palmilhas planas no grupo controle), no entanto, relatou que o uso de anti-inflamatórios não esteroidais diminuiu por parte do grupo que utilizou palmilhas com cunha lateral. Conclusão similar a da revisão da literatura realizada por Gélis et al (2005) e por Brouwer (2005).
Toda et al (2002) já havia relatado que o uso desse tipo de correção em palmilhas leva ao realinhamento do ângulo fêmorotibial e mostra que a adição de enfaixamento subtalar torna essas órteses mais eficientes em indivíduos mais jovens.
Baker e colaboradores (2007), ao contrário, não encontraram diferenças estatisticamente relevantes no Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) ou clinicamente importantes ao realizar um ensaio com 90 pacientes com OAJ.
Pé Diabético:
A neuropatia periférica diabética (NPD) é uma das complicações mais comuns associadas à diabetes mellitus, agrupa uma série de sinais clínicos e subclinicos com etiologia e manifestações variadas (Picon 2012) e é definida pela degeneração progressiva, difusa ou não, das fibras nervosas periféricas somáticas e sensoriais (Greene 1992).
Acredita-se que aproximadamente 50% das pessoas com diabetes vão desenvolver esse quadro entre 10 e 15 anos de doença (Bacarin 2009).
Dos 11 artigos encontrados sobre o uso de calçados e órteses plantares em diabéticos, cinco são ensaios clínicos que abordam o alivio de pontos de pressão plantar na tentativa de tratar ou evitar ulcerações.
Lobmann e colaboradores (Lobmann 2001) em seu ensaio clínico estudaram 81 pacientes diabéticos sem lesão plantar, todos submetidos inicialmente a baropodometria durante a marcha, divididos em dois grupos: o grupo intervenção no qual os pacientes com risco de desenvolver úlceras plantares segundo o pico de pressão plantar recebiam palmilhas de EVA, polietileno e silicone e o grupo controle, o qual recebeu somente calçado convencional.
Eles descrevem a redução de 30% dos valores de pressão total nos pés com o uso de palmilhas, no entanto, após seis meses de tratamento as pressões voltaram a aumentar. No grupo controle foi notado o aumento significativo dos picos de pressão em todas as regiões do pé. Eles concluem que o uso dessa órtese plantar é eficiente na redução das pressões plantares e que ajustes devem ser feitos a cada 6 meses nas palmilhas.
Caravaggi et al (2000) testaram os efeitos de órteses de fibra de vidro no tratamento de úlceras plantares no pé diabético realizando um ensaio clínico controlado no qual o grupo controle recebeu calçados de solado rígido para diabéticos com palmilhas de plastazote.
Ambos os grupos tiveram a área das lesões mensurada e acompanhada por 30 dias. A porcentágem de lesões completamente curadas após 30 dias foi de 50% no grupo que recebeu órteses de fibra de vidro contra 20,8% no grupo que utilizou os calçados para diabéticos. Além disso, nenhuma nova lesão surgiu nos indivíduos do grupo intervenção enquanto dois sujeitos desenvolveram novas úlceras plantares.
Bus et al(2011) compararam os valores de pressão plantar e a integral da força no tempo em 20 pacientes diabéticos que utilizavam palmilhas customizadas ou pré fabricadas planas, encontrando reduções de ambos parâmetros nos usuários de palmilhas customizadas sob a cabeça dos metatarsos e sob os calcanhares. Esses parâmetros tiveram aumento dos valores sob o médio pé no caso das palmilhas personalizadas enquanto, nas pré-fabricadas, não houve alteração.
Quanto ao tipo de calçado, Charanya e colaboradores (2004) pesquisaram os efeitos da dureza do solado e espessura dos calçados na distribuição das pressões plantares em diabéticos neuropatas. Seus resultados mostraram aumentos de até 2,5 vezes nos valores de pressão plantar para solados com valores de densidade mais elevados (level de shore 30-40 comparados aos shore 20-30). Propõem ainda a escolha da densidade da sola e palmilha dos sapatos em relação aos valores de sensibilidade plantar em mN.
Um estudo de Hall (2004) parte do principio que a formação de úlceras plantares advém do aumento da temperatura nos tecidos moles da região, ocasionando em lesão desses tecidos. Realizou então um ensaio clinico no qual se aferiu a temperatura dos pés de 13 adultos saudáveis com um termômetro infravermelho utilizando palmilhas com sete materiais diferentes: Bocklite, Pe-Lite, Plastazote, Poron, Poron forrado do Nylon, EVA Ortholite e um tri-laminado Ortholite/Poron/Ortholite.
Hall encontra em seus resultados que não houve diferença de temperatura nas regiões dos pés quando comparados os diferentes materiais ou seja, o aumento da temperatura plantar nos indivíduos saudáveis não foi amenizada por nenhum material testado.
Hallux Valgus:
Hallux Vagus é o distúrbio que se manifesta com o desvio lateral do primeiro dedo e desvio medial do primeiro metatarso de alta prevalência em mulheres na quarta, quinta e sexta década de vida.
De etiologia multifatorial, aparentemente o uso de calçados apertados é a maior causa extrínseca, embora fatores intrínsecos tenham sido amplamente propostos. Teorias como a pronação do retropé e pés tipo plano tem sido sugeridas e ainda o aumento do ângulo entre o primeiro e o segundo metatarso (metatarsus primus varus) é comumente associado ao HV (Inman 1974, Mann 1981).
Tang et al. realizaram um ensaio clinico avaliando 17 pacientes com halux valgo doloroso num estudo sem grupo controle testando uma palmilha customizada contato total com separador de dedos feita em material plástico e plastazote (Tehraninasr 2008). Os dados coletados foram a escala visual analógica de dor (NRS-11) e uma escala modificada de Pun para avaliação da habilidade de marcha.
Após três meses os sujeitos foram reavaliados e se constatou melhora estatisticamente significativa tanto na habilidade de marcha quanto no índice de dor. Os autores ainda relataram uma diminuição no ângulo de valgismo do hálux ao fim do estudo, concluindo que a ortese desenvolvida pode ser considerada um método eficaz o tratamento de pacientes com hálux valgo doloroso.
Fascite Plantar:
Fascite plantar é a inflamação do tecido denso e resistente que recobre a musculatura da planta dos pés. Condição auto-limitante, é causa comum de dor no calcanhar em adultos e afeta mais de um milhão de pessoas por ano. Geralmente relacionada com obesidade, pronação excessiva, excesso de corrida ou bipedestação prolongada (Goff 2011), pode também ser resultado de déficit de estabilidade e de um bom apoio do calcanhar, ou pelo ponto de flexibilidade inadequado(Cohen 2003). O tratamento conservativo é baseado em repouso, crio massagem, antiinflamatório não esteroidal, analgésico, injeção, alongamento, uso de órtese customizada ou não e tala noturna. Em casos que perduram por seis meses ou mais, a opção é a terapia com ondas de choque ou a fasciotomia. Em geral, o tratamento conservativo é eficiente em 90% dos casos(Goff 2011, Neufeld 2008).
Foram encontrados dois artigos na literatura sobre uso de órteses na fascite plantar.
Williams (1987) descreve que na maioria dos quadros que apresentam dores calcâneas respondem bem a órteses com preenchimento macio no calcanhar.
Neufeld (2008) relatou que embora o tratamento utilizado atualmente para fascite plantar não se baseie em evidências científicas, o uso de combinações das técnicas de alongamento, talas noturnas, fisioterapia, massagem, palmilhas customizadas ou pré-fabricadas e injeções com anti-inflamatórios tendem a solucionar o problema em cerca de 90% das vezes.
Fratura por Estresse:
A fratura por estresse resulta de uma carga cíclica e repetitiva sobre a estrutura óssea e que supera a capacidade de reparação do sistema esquelético. Difere das demais fraturas por não resultar de evento traumático agudo sendo mais comum entre atletas e militares e atingindo principalmente atletas do sexo feminino (Cohen 2003, Reeder 1996, Patel 2011). Dentre os fatores de risco, encontram-se aspectos biomecânicos e ambientais. A idade, sexo, raça, o nível de atividade e de condicionamento físico, distúrbio hormonal (hipoestrogenismo), desequilíbrios alimentares (bulimia e anorexia) e as características biomecânicas (assimetrias) são fatores que predispõe à fratura por estresse (Cohen 2003).
Ocorrem mais comumente em membros inferiores e apresentam distribuição percentual aproximada do total de locais anatômicos acometidos da seguinte maneira: tíbia com 50%, ossos do tarso 25%, metatarsos 8,8%, fêmur 7,2%, fíbula 6,6%, pelve 1,6% e sesamóides 0,9% (Cohen 2003).
O tratamento é, na maioria dos casos, conservador e consiste em repouso, mudança ou pausa na atividade física, diminuição da descarga de peso no membro acometido com uso de muleta, uso de analgésicos e brace pneumático 102,103. Em caso de recorrência, não consolidação óssea ou fratura em local de alto risco, a cirurgia é indicada (Patel 2011).
Mattila et al (2011) realizaram um ensaio clinico randomizado e controlado para verificar se palmilhas ortopédicas são capazes de prevenir lesões por overuse em membros inferiores.
Para tal, 228 sujeitos foram divididos em dois grupos. O primeiro receberia palmilhas customizadas tipo contato total e o segundo seria o grupo controle. Ambos praticariam atividade física e seriam avaliados clinicamente por um médico. O estudo não encontrou diferença entre os grupos, ou seja, não houve diferença significativa no número de pacientes diagnosticados com lesões por overuse entre os grupos.
Withhnall (Withnall 2006) encontrou resultados similares aos de Mattila em recrutas da aeronáutica ao comparar o uso de diferentes materiais para palmilhas planas: Saran (controle), Sorbotano e Poron. Nenhuma diferença no número de diagnósticos de lesões nos grupos foi encontrada. Gardner em 1988 chegou a mesma conclusão utilizando palmilhas de polímero viscoelástico.
No entanto, House e colaboradores (2004) encontraram reduções nos picos de pressão durante a corrida ao se utilizar palmilhas para absorção de impactos em recrutas do exército usando botas militares. Já Windle (1999) em um estudo similar encontrou redução significativa nas pressões plantares durante a marcha e corrida com o uso de palmilhas de sorbotano.
Artrite Reumatoide:
A artrite reumatoide (AR) é uma doença autoimune de etiologia desconhecida que se expressa como inflamação sistêmica e culmina em deformidades articulares, perda de funcionalidade e dor. O pé é o sítio inicial da expressão dos sintomas em um terço dos pacientes com artrite reumatoide e até 85% desses pacientes evoluem com comprometimentos nos pés durante o curso da doença (Oishi 2011).
Oishi e colaboradores (2011) fizeram uma revisão na literatura no objetivo de identificar a efetividade e o nível de evidência do uso de órteses plantares em adultos com artrite reumatoide. Quinze artigos cumpriram os critérios de inclusão e foram reportados em termos do tipo de tratamento e resultados.
Como resultado, é relatado que há evidência consistente que o uso de órteses plantares reduz a dor e melhora a funcionalidade de pacientes com AR.
A prescrição de órteses plantares rígidas tiveram bons resultados quanto a redução da dor nos pés (avaliado pela escala visual analógica) em sete estudos, reduzindo a progressão de halux valgo em 5 estudos avaliados e resultados positivos na biomecânica da marcha em um dos estudos. No entanto, em 5 dos artigos encontrados as evidências encontradas quanto a estabilização do quadro álgico e das deformidades são inconclusivas.
O uso de órteses macias também resultou em redução de dor segundo três artigos reportados e acredita-se que parte disso ocorre pela redistribuição da pressão plantar. Ainda foram descritos o aumento do comprimento do passo e passada com o uso de barras retrocapitais e pilotos. Somente um dos artigos relata que o uso desse tipo de órtese não resulta em modificações significativas na função ou nível de dor em pacientes com AR.
Quanto as órteses semi-rígidas, em quatro estudos foram encontradas melhoras na dor nos pés dos pacientes com AR mas nenhuma alteração em parâmetros antropométricos ou biomecânicos da marcha.
As órteses customizadas não apresentaram resultados consistentes segundo cinco artigos que relataram benefícios quanto à dor nos pés sem significância estatística para pacientes com AR.
Sesamoidite:
Os sesamóides são ossos de formação embrionária na quinta semana de desenvolvimento fetal, com centro cartilaginoso, e não por formação articular. Estão incrustados em tendões específicos: o sesamóide metatarso falangeano medial está interno ao tendão da cabeça medial do flexor curto do hálux e o sesamóide lateral, no tendão lateral do flexor curto do halux.
Os ossos sesamóides interfalangeanos são encontrados dentro dos tendões do flexor longo do hálux e dos demais dedos, nos lumbricais.
São firmemente ligados entre si por ligamentos intersesamoideanos (Jahss 1981, Vanore 2003).
Somente um estudo foi encontrado citando a utilização de órteses plantares para sesamoidite. Segundo Leventen (1991), o tratamento da sesamoidite deve sempre se iniciar pela forma conservadora, utilizando-se palmilhas moldadas com depressões para deslocar os pontos de pressão elevados do sesamóide doloroso.
Os benefícios da abordagem cirúrgica variam com a técnica utilizada, visto a possibilidade do desenvolvimento de dedos em garra ou lesões nervosas por iatrogenia.
Discussão:
Embora diversos estudos tenham sido encontrados sobre o uso de órteses plantares e palmilhas ortopédicas na pratica clínica, a distribuição desses estudos parece pouco relacionada à importância da patologia em relação a sua ocorrência na população.
O maior número de artigos encontrados se relacionava a osteoartrite de joelhos e pés diabéticos, que obviamente são síndromes de grande importância e alta incidência na população. Tais estudos pertenciam em sua maioria mesmo grupo de cientistas, revelando mais a competência do grupo que o interesse real da comunidade científica nesse tipo de abordagem.
No entanto, poucos estudos foram encontrados em referência a alguns agravos nos quais usualmente se prescreve o uso de órteses plantares como neuroma de morton, metatarsalgia, fasciite plantar e hálux valgo.
Outros problemas abundantes na população nos quais comumente é prescrito o uso de palmilhas ortopédicas são as deformidades adquiridas como coalisão tarsal e dedos em garra ou martelo, diferenças de comprimento de membros inferiores de etiologias diversas, diferentes síndromes de déficit sensorial plantar e hiperqueratoses.
Entretanto, para essas moléstias não foi encontrado estudo de nenhum tipo.
Conclusão:
Embora a maioria dos estudos careça de qualidade metodológica e detalhes da objetivos da construção das órteses, a literatura aponta certas tendências.
Não foi encontrado em nenhum estudo indicando que o uso de órteses plantares agravaram ou implicaram em novas moléstias.
A maioria dos estudos apontou satisfação do paciente com as órteses e melhora nas dores mesmo quando os resultados confirmavam as hipóteses nulas ao que se refere aos estudos tipo caso-controle. Esse fato também pode apontar a coleta de pequeno número amostral ou a investigação de variáveis não correlatas, apontando a necessidade de uma nova abordagem. Como exemplo as alterações nas pressões plantares em pacientes com fraturas por estresse obtidas por palmilhas, mas sem resultados clínicos de melhora.
A literatura carece de estudos do tipo ensaio clínico com palmilhas e outras órteses no tratamento de moléstias muito incidentes como neuroma de Morton, sesamoidite, deformidades adquiridas dos dedos e dos pés e fascite plantar.
Por outro lado, os achados científicos desse tipo de tratamento na osteoartrite e fraturas por estresse nos metatarsos, embora abundantes, são pouco difundidos.
Também um novo ramo de investigações na neurologia sobre a resposta cortical e muscular local a estímulos cutâneos plantares esboça uma utilidade diferente em pacientes com sequelas neurológicas.
Após essa investigação da literatura, pode-se concluir que é necessária uma melhor orientação quanto aos trabalhos científicos realizados sobre órteses plantares.
Anexo 1: Tabela de Artigos
Artigos sobre Diabetes:
| Autor e ano | Tipo de estudo | Tema | Intervenção | Outcome measures | Resultados |
| Paton 2011 | Revisão | Órtese plantar no paciente com neuropatia diabética | Órtese plantar na prevenção de úlcera no pé diabético | Não se aplica | Há um número pequeno de evidências que comprovem a eficácia da palmilha |
| Cavanagh 2006 | Revisão | Pé diabético | Não se aplica | Não se aplica | Órtese customizada pode diminuir a pressão plantar |
| Inlow 1999 | Revisão | Métodos para diminuir pressão plantar em pacientes com diabetes | Tratamento cirúrgico x tratamento conservador | CarvilleClassification System | Não se aplica |
| Janisse 1995 | Revisão | Órtese plantar e calçado em pacientes com diabetes | Não se aplica | Não se aplica | Redução da pressão plantar, mas ainda há pouca evidência |
| Bus 2011 | Ensaio clínico | Calçados customizados para pacientes com neuropatia diabética | Modificação do calçado ou palmilha conforme o pico de pressão | Mensuração da pressão plantar | Pico de pressão plantar reduziu significativamente |
| Van Geffen 2007 | Ensaio clínico | Órtese em pacientes com neuropatia diabética | Órteses com diferentes bordas x grupo controle | Estabilidade postural em quatro diferentes condições | Não houve efeito negativo com a órtese de borda baixa |
| Charanya 2004 | Ensaio clínico | Pressão plantar em pacientes com neuropatia diabética | Não se aplica | Não se aplica | Não se aplica |
| Hall 2004 | Ensaio clínico | Órtese e temperatura plantar | Seis tipos de órteses de materiais diferente foram testados | Temperatura do hálux, cabeça do 1° e 5° metatarso, calcanhar e bíceps contralateral | Diferença significativa em todos os materiais, em relação a temperatura inicial |
| Bus 2004 | Ensaio clínico | Órtese customizada em pacientes com neuropatia diabética | Órtese customizada x órtese plana | Pico de pressão e tempo de força | Órtese customizada é mais efetiva na diminuição de carga |
| Lobmann 2001 | Ensaio clínico | Órtese plantar customizada em pacientes com diabetes | Órtese plantar customizada x grupo controle | Pico de pressão plantar máximo, do calcanhar e da cabeça do metatarso | Eficaz na redução da pressão plantar em 6 meses |
| Caravaggi 2000 | Ensaio clínico | Tratamento para úlcera neuropática de pé | Calçado especializado com solado rígido e órtese alkaform x fiberglass cast | Área da úlcera | Resolução mais rápida com o fiberglass cast |
| Kastenbauer 1998 | Ensaio clínico | Pressão plantar em pacientes com diabetes | Órtese plantar customizada x diferentes calçados | Pressão plantar | Houve redução da pressão plantar, principalmente no caso da órtese customizada |
| Reiber 1997 | Ensaio clínico | Teste de sistema de calçado para pacientes com diabetes | Calçado customizado com diferentes órteses | Risco de ulceração | Não houve sinal de lesão na pele em nenhum dos casos |
Artigos sobre Osteoartrite:
| Autor e ano | Tipo de estudo | Tema | Intervenção | Outcome measures | Resultados |
| Gélis 2005 | Revisão | Órtese plantar e OA de joelho | Não se aplica | Não se aplica | Órtese plantar é uma alternativa de tratamento não farmacológico para OA de joelho, mas há pouca evidência. |
| Brouwer 2005 | Revisão | Brace de joelho e órtese plantar em paciente com OA de joelho | Não se aplica | WOMAC, MACTAR e VAS | Alternativa para redução da dor, mas há pouca evidência. |
| Turpin 2012 | Ensaio clínico | Ortese com absorção de impacto em pacientes com osteoartrite de joelho | Uso diário de ortese durante um mês | Pico nas fases da marcha e pico do KAM, WOMAC índex pain subscale | Redução significativa da dor e disfunção no joelho |
| Fantini Pagani 2012 | Ensaio clínico | Brace de joelho e ortese plantar em pacientes com osteoartrite de joelho | Órtese de joelho em dois ângulos de valgo e órtese plantar lateral | Análise de movimento e plataforma de força | Órtese de joelho foi mais efetivo na redução do KAM |
| Van Raaij 2010 | Ensaio clínico | Ortese plantar e brace de joelho em pacientes com osteoartrite de joelho | Uso de ortese plantar lateral x uso de brace de joelho | Escala visual analógica de dor, WOMAC score, correção do varo por RX e OMERACT-OARSI criteria. | Pequena diferença entre os grupos, sendo que o uso da ortese apresentou melhor resposta. |
| Hinman 2009 | Ensaio clínico | Ortese plantar lateral em pacientes com osteoartrite de joelho | Calçado com órtese plantar lateral x grupo controle | 1° e 2° pico do momento de adução do joelho e angulação | Redução significativa do momento de adução. |
| Segal 2009 | Ensaio clínico | Suporte de tornozelo com órtese plantar lateral em pacientes com osteoartrite de joelho | Uso de órtese plantar lateral antes ou depois do uso com suporte de tornozelo | Alinhamento do MI, ângulo de inclinação talocalcâneo e talar, carga no compartimento medial, escala visual analógica de dor e Knee Osteoarthritis Outcome Score | Uso simultâneo de órtese e suporte para tornozelo não melhora o alinhamento mecânico ou a carga no compartimento medial |
| Rodrigues 2008 | Ensaio clínico | Órtese em pacientes com OA de joelho | Órtese medial x órtese neutra | VAS, WOMAC; ângulo femorotibial e talocalcâneo | Redução da dor e melhora funcional do valgo de joelho com a órtese medial |
| Toda 2008 | Ensaio clínico | Calçado com salto e órtese plantar lateral em pacientes com OA de joelho | Órtese com ou sem calçado x órtese com faixa, com ou sem calçado x grupo controle | Lequesne índex score | Órtese plantar lateral apresenta melhor resultado sem calçado com salto |
| Baker 2007 | Ensaio clínico | Órtese plantar lateral em pacientes com OA de joelho | Órtese plantar lateral x grupo controle | WOMAC, EVA, teste do sentar-levantar, 50-feet walk time | Não houve resultado significativo |
| Kuroyanagi 2007 | Ensaio clínico | Órtese plantar lateral com faixa subtalar em pacientes com OA de joelho | Descalço x órtese convencional x faixa subtalar | Pico do momento de varo do joelho | Faixa subtalar apresentou melhor efeito na redução do pico de momento |
| Shimada 2006 | Ensaio clínico | Órtese plantar lateral em pacientes com OA de joelho | Grupo OA x grupo controle | Pico do KAM, Kellgren and Lawrence grading system | Significativo efeito cinético e cinemático |
| Toda 2006 | Ensaio clínico | Órtese plantar em pacientes com OA de joelho | Órtese subtalar com faixa x órtese plantar tradicional | Medida do ângulo femorotibial por RX e Lequesne index | Mudança significativa no ângulo femorotibial com órtese subtalar após dois anos |
| Toda 2005 | Ensaio clínico | Órtese plantar em pacientes com OA de joelho | Órtese subtalar com faixa x grupo controle | Ângulo femorotibial e Lequesne índex | Correção do valgo no grupo teste, principalmente com uso entre 5 e 10h diárias |
| Toda 2004 | Ensaio clínico | Órtese plantar em pacientes com OA de joelho | Órtese plantar com faixa subtalar x órtese plantar tradicional | Ângulo femorotibial, VAS e Lequesne índex | Melhora significante no grupo com faixa subtalar, após 6 meses |
| Toda 2004 | Ensaio clínico | Órtese plantar lateral com faixa subtalar em pacientes com OA de joelho | Órtese plantar lateral com faixa subtalar com três elevações diferentes | Ângulo femorotibial por RX e Lequesne índex | Melhor efeito com as órteses de 8 ou 12mm |
| Pham 2004 | Ensaio clínico | Órtese plantar com elevação lateral em pacientes com OA de joelho | Órtese plantar lateral x grupo controle | Assessment of disease activity e WOMAC índex subscale | Não houve efeito sintomático e/ou estrutural |
| Toda 2002 | Ensaio clínico | Órtese plantar em pacientes com OA de joelho | Órtese plantar com faixa elástica subtalar x suporte de tornozelo com cunha lateral de calcanhar | Ãngulo femorotibial por RX e Lequesne índex | Melhora biomecância e sintomática, com faixa subtalar |
| Toda 2002 | Ensaio clínico | Composição corporal e órtese plantar em pacientes com OA de joelho | Órtese com faixa subtalar x órtese com faixa talonavicular | Angulo femorotibial por RX, L-LBM, Kellgren-Lawrence e Lequesne index | Órtese com faixa subtalar é mais eficaz em pacientes jovens e com alto L-LBM por peso corporal |
| Maillefert 2001 | Ensaio clínico | Órtese plantar com elevação lateral em pacientes com OA de joelho | Órtese plantar lateral x grupo controle | Assessment of disease activity e WOMAC índex subscale | Não houve efeito sintomático a curto prazo |
| Toda 2001 | Ensaio clínico | Órtese subtalar em pacientes com OA de joelho | Órtese com faixa elástica subtalar x grupo controle | Ângulo femorotibial e talar por RX, VAS | Diminuição dos ângulos e da dor no grupo teste |
Fratura por Estresse:
| Autor e ano | Tipo de estudo | Tema | Intervenção | Outcome measures | Resultados |
| Anderson 1990 | Revisão | Órtese plantar na fratura por estresse do pé | Não se aplica | Não se aplica | Correção biomecânica |
| Mattila 2011 | Ensaio clínico | Uso de palmilha ortopédica na prevenção de lesão por overuse | Palmilha ortopédica x grupo controle | Diagnóstico médico de lesão e Modelo de Regressão de Cox | Não há associação entre uso de palmilha ortopédica e diminuição de lesão por overuse em MMII |
| Gardner 1988 | Ensaio clínico | Órtese com absorção de impacto na fratura por estresse | Órtese de polímero x órtese padrão | Incidência de lesão por estresse; idade e custo do calçado | Mesmo a órtese com alta absorção de impacto não preveniu a reação por estresse em recrutas da marinha |
Análise de Pressão Plantar:
| Autor e ano | Tipo de estudo | Tema | Intervenção | Outcome measures | Resultados |
| Ki 2008 | Ensaio clínico | Órteses na pressão plantar | Órtese simples x órteses customizadas | Novel Pedar-mobile in-shoe | Redução do pico de pressão e da força máxima no calcanhar com órteses customizadas |
| Withnall 2006 | Ensaio clínico | Órtese plantar com absorção de impacto | Órteses com absorção de impacto x órtese sem absorção de impacto | Lesão em membros inferiores, diagnóstico médico | Observou-se taxa similar de lesão em MI em todos os grupos |
| House 2004 | Ensaio clínico | Órtese com absorção de impacto | Órteses com diferentes espessuras x grupo controle | Pressão plantar | Diminuição do pico de pressão no calcanhar e antepé, no uso das órteses |
| House 2002 | Ensaio clínico | Órtese e pico de pressão plantar | Órtese plantar x grupo controle | Pressão plantar do calcanhar e antepé | Redução da pressão plantar durante corrida com bota militar |
| Redmond 2000 | Ensaio clínico | Órtese na pressão e força plantar | Calçado atlético x órtese plantar | Pressão e força plantar | Òrtese moldada apresentou diminuição da força e pressão no calcanhar |
| Windle 1999 | Ensaio clínico | Órtese na pressão plantar | Órteses plantar x grupo controle | Pressão plantar no calcanhar e antepé | Diminuição da pressão no grupo teste |
| Randolph 1999 | Ensaio clínico | Órtese na pressão plantar | Caminhada com diferentes tipos de calçados e com órtese | Pressão no antepé, mediopé e retropé | Redistribuição da pressão plantar com calçado de solado plano e de solado rocker |
Prática de Esporte:
| Autor e ano | Tipo de estudo | Tema | Intervenção | Outcome measures | Resultados |
| Shin 2011 | Ensaio clínico | Uso de ortese em corredores com pé pronado | Ortese x grupo controle | 60-minutes treadmill test | Redução imediata na incidência de dor no grupo intervenção |
| O’Leary 2008 | Ensaio clínico | Órtese almofadada em corredores | Uso de órtese x não uso | Força de reação do solo, aceleração tibial, cinemática do MI e relato de conforto | Eficácia na redução do pico de força de impacto e na aceleração tibial |
Equilíbrio e instabilidade:
| Autor e ano | Tipo de estudo | Tema | Intervenção | Outcome measures | Resultados |
| Maki 2011 | Revisão | Queda em idosos | Não se aplica | Não se aplica | Não se aplica |
| Perry 2008 | Ensaio clínico | Órtese plantar no controle do equilíbrio | Órtese convencional x órtese facilitatória | Protocolo de perturbação de marcha | Melhora do equilíbrio lateral na marcha e diminuição de queda com órtese facilitatória |
| Waddington 2003 | Ensaio clínico | Órtese plantar na inversão de tornozelo | Sem calçado x chuteira x chuteira com órtese | Ankle movement extent discrimination apparatus (AMEDA) | O uso de órtese melhora o feedback sensorial |
Fascite Plantar:
| Autor e ano | Tipo de estudo | Tema | Intervenção | Outcome measures | Resultados |
| Williams 1987 | Revisão | Calcanhar doloroso | Não se aplica | Não se aplica | Redução da dor por órtese customizada |
| Caselli 1997 | Ensaio clínico | Órtese em pacientes com dor no calcanhar | Órtese moldada com folha magnética x sem a folha magnética | Foot function index | Houve melhora, mas sem diferença significativa entre os grupos |
Outros Artigos:
| Autor e ano | Tipo de estudo | Tema | Intervenção | Outcome measures | Resultados |
| Schreiber 2011 | Revisão | Neuroma de Morton | Não se aplica | Não se aplica | Não se aplica |
| Hossain 2011 | Revisão | Orteses em pacientes com dor patelofemoral | Estudos comparativos de ortese x palmilha comum x fisioterapia | Não se aplica | Não há diferença significativa entre ortese x fisioterapia |
| Leventen 1991 | Revisão | Órtese customizada em pacientes com sesamoidite | Não se aplica | Não se aplica | Redução da pressão e dor |
| Ferrari 2012 | Ensaio clinico | Orteses customizadas em pacientes com fibromialgia | Orteses plantares personalizadas x grupo controle | Revised Fibromyalgia Impact Questionnaire | Melhora da funcionalidade em curto prazo |
| Kutzner 2011 | Ensaio clínico | Efeito de calço lateral no compartimento medial do joelho | Órtese com e sem estabilização de tornozelo x grupo controle | Força de contato tibiofemoral medial | Redução do pico de força no compartimento medial do joelho |
| Sungkarat 2011 | Ensaio clínico | Palmilha em pacientes pós AVE | Uso de palmilha e sensor de pressão durante a marcha x grupo controle | Velocidade da marcha, comprimento do passo, tempo de apoio unipodálico, equilíbrio e carga no membro parético durante a postura | Aumento da simetria durante postura e marcha, melhora da velocidade da marcha e do equilíbrio |
| Perhamre 2011 | Ensaio clínico | Uso de órtese na doença de Sever | Comparação entre dois tipos de órtese para calcanhar | Escala de dor | Redução da dor nos dois grupos; heel cup apresentou melhor resultado |
| Hartmann 2010 | Ensaio clínico | Palmilha em pacientes idosos | Grupo treino x grupo treino com palmilha x grupo controle | Falls Efficacy Scale- International, análise de marcha e força muscular de MMII | Não há diferença, há longo prazo, no uso ou não de palmilha |
| Cho 2009 | Ensaio clínico | Órtese plantar com tênis especializado em pacientes com artrite reumatoide de pé | Órtese plantar customizada e semi-rígida x órtese plantar pronta e macia | Escala visual analógica de dor, Foot Function Index, quantidade de medicamentos e articulações ativas | Houve melhora nos dois grupos, mas sem diferença significativa entre eles |
| Nakajima 2009 | Ensaio clínico | Uso de suporte de arco plantar com órtese plantar lateral | Órtese plana com e sem suporte para arco x órtese com inclinação lateral com e sem suporte para arco | Parâmetros cinéticos e cinemáticos do joelho e articulação subtalar | Uso de suporte de arco plantar com órtese lateral reduziu o momento de adução do joelho |
| Ciuffolo 2006 | Ensaio clínico | Órtese plantar na ativação muscular e postura | Órtese plantar x grupo controle | Eletromiografia e plataforma de força | Aumento da ativação muscular no grupo teste |
| Branthwaite 2004 | Ensaio clínico | Órtes plantar simples na marcha normal | Órteses simples x grupo controle | Posição do antepé e retropé, rotações do pé em três eixos ortogonais | Não houve efeito significativo das órteses na pronação excessiva do pé |
| Gillespie 2003 | Ensaio clínico | Órtese plantar no impacto durante a marcha | Caminhada sem calçado sobre plataforma de força, com órteses sobre a superfície | Filterbank program | Diminuição do impacto durante a marcha |
| Ogon 2001 | Ensaio clínico | Órtese plantar na dor lombar | Corrida sem calçado x com tênis atlético | Força de reação do solo, aceleração no 3° nível lombar e ativação do eretor espinal | Melhora estabilização lombar interna |
| Uchio 2000 | Ensaio clínico | Órtese plantar lateral em pacientes com osteonecrose de joelho | Órtese plantar x grupo controle | Knee score | Melhora significativa no grupo teste com diminuição da área necrótica |
| Crenshaw 2000 | Ensaio clínico | Órtese plantar lateral na cinética do joelho | Marcha com órtese plantar lateral e sem | Análise de movimento e plataforma de força | Diminuição do momento de varo do joelho e da carga medial |
| Postema 1998 | Ensaio clínico | Metatarsalgia | Órtese comum, órtese customizada e rockerbar em 4 combinações diferentes | Pressão plantar | Órtese customizada e a rockerbar, diminuíram o pico de pressão e força |
| Caselli 1997 | Ensaio clínico | Órtese em pacientes com hiperqueratose submetatarsal | Debridamento para todos os grupos; Órteses plantar x grupo controle | Foot function índex | Houve melhora para os dois tipos de órtese |
| Seboka 1996 | Ensaio clínico | Calçado para pacientes com hanseníase | Sapato de lona x sapato moldado plastazote | Presença de úlcera | Sujeitos que usaram o sapato de lona não tinham mais úlcera após um ano |
| Jackson 2004 | Ensaio clínico | Órtese pré-fabricada em pacientes com artrite reumatoide | Òrteses pré-fabricadas com coxim metatarsal x grupo controle | Pressão plantar | Diminuição do pico de pressão plantar no grupo teste |
Referências Bibliográficas:
- – Schreiber K, Khodaee M, Poddar S, Tweed EM. Clinical Inquiry. What is the best way to treat Morton’s neuroma? J Fam Pract. 2011 Mar;60(3):157-8, 168.
- – Caselli MA, Clark N, Lazarus S, Velez Z, Venegas L. Evaluation of magnetic foil and PPT Insoles in the treatment of heel pain. J Am Podiatr Med Assoc. 1997 Jan;87(1):11-6.
- – Benvenuti F, Ferrucci L, Guraunik JM, Gangemi S, Baroni A. Foot pain and disability in older persons: an epidemiologic survey. J Am Geriatr Soc. 1994. 43:479-484.
- – Withnall R, Eastaugh J, Freemantle N. Do shock absorbing insoles in recruits undertaking high levels of physical activity reduce lower limb injury? A randomized controlled trial. J R Soc Med. 2006 Jan;99(1):32-7.
- – Van Geffen JA, Dijkstra PU, Hof AL, Halbertsma JP, Postema K. Effect of flat insoles with different Shore A values on posture stability in diabetic neuropathy. Prosthet Orthot Int. 2007 Sep;31(3):228-35.
- – Oishi A, Prior M, Worley A. The use of foot orthoses in the management of rheumatoid arthritis patient. The internet journal of allied health sciences and practice; 2011.
- – Jahss MH. The Sesamoids of the Hallux.Current Orthopaedic Practice. 1981:157:88-97
- – Biblioteca Virtual em Saúde (BVS). Site da web: http://regional.bvsalud.org
- – Medical Subject Headings. US National Library of Medicine. Pagina da Web: http://www.nlm.nih.gov/mesh/
- – Postema K, Burm PE, Zande ME, Limbeek Jv. Primary metatarsalgia: the influence of a custom moulded insole and a rockerbar on plantar pressure. Prosthet Orthot Int. 1998 Apr;22(1):35-44.
- – Spina R, Cameron M, Alexander R. The effect of functional fascial taping on Morton’s neuroma. ACO 2002;10: 45-50.
- – Toda Y, Tsukimura N. A six-month followup of a randomized trial comparing the efficacy of a lateral-wedge insole with subtalar strapping and an in-shoe lateral-wedge insole in patients with varus deformity osteoarthritis of the knee. Arthritis Rheum. 2004 Oct;50(10):3129-36.
- – van Raaij TM, Reijman M, Brouwer RW, Bierma-Zeinstra SM, Verhaar JA. Medial knee osteoarthritis treated by insoles or braces: a randomized trial. Clin Orthop Relat Res. 2010 Jul;468(7):1926-32.
- – Shimada S, Kobayashi S, Wada M, Uchida K, Sasaki S, Kawahara H, Yayama T, Kitade I, Kamei K, Kubota M, Baba H. Effects of disease severity on response to lateral wedged shoe insole for medial compartment knee osteoarthritis. Arch Phys Med Rehabil. 2006 Nov;87(11):1436-41.
- – Pham T, Maillefert JF, Hudry C, Kieffert P, Bourgeois P, Lechevalier D, Dougados M. Laterally elevated wedged insoles in the treatment of medial knee osteoarthritis. A two-year prospective randomized controlled study. Osteoarthritis Cartilage. 2004 Jan;12(1):46-55.
- – Gélis A, Coudeyre E, Aboukrat P, Cros P, Hérisson C, Pélissier J. Feet insoles and knee osteoarthritis: evaluation of biomechanical and clinical effects from a literature review. Ann Readapt Med Phys. 2005 Dec;48(9):682-9. Epub 2005 Jun 13.
- – Brouwer RW, Jakma TS, Verhagen AP, Verhaar JA, Bierma-Zeinstra SM. Braces and orthoses for treating osteoarthritis of the knee. Database Syst Rev. 2005 Jan 25;(1)
- – Baker K, Goggins J, Xie H, Szumowski K, LaValley M, Hunter DJ, Felson DT. A randomized crossover trial of a wedged insole for treatment of knee osteoarthritis. Arthritis Rheum. 2007 Apr;56(4):1198-203.
- – Greene DA, Sima AAF, Stevens MJ, Feldman EL, Lattimers A. Complications: neuropathy, pathogenic considerations. Diabetes Care. 1992;15:1902-25.
- – Bacarin TA, Sacco ICN, Hennig EM. Plantar pressure distribution patterns during gait diabetic neuropathy patients with a history of foot ulcers. Clinics 2009;64(2):113-20.
- – Lobmann R, Kayser R, Kasten G, Kasten U, Kluge K, Neumann W, Lehnert H. Effects of preventative footwear on foot pressure as determined by pedobarography in diabetic patients: a prospective study. Diabet Med. 2001 Apr;18(4):314-9.
- – Caravaggi C, Faglia E, De Giglio R, Mantero M, Quarantiello A, Sommariva E, Gino M, Pritelli C, Morabito A. Effectiveness and safety of a nonremovable fiberglass off-bearing cast versus a therapeutic shoe in the treatment of neuropathic foot ulcers: a randomized study. Diabetes Care. 2000 Dec;23(12):1746-51.
- – Bus SA, Haspels R, Busch-Westbroek TE. Evaluation and optimization of therapeutic footwear for neuropathic diabetic foot patients using in-shoe plantar pressure analysis. Diabetes Care. 2011 Jul;34(7):1595-600.
- – Charanya G, Patil KM, Narayanamurthy VB, Parivalavan R, Visvanathan K. Effect of foot sole hardness, thickness and footwear on foot pressure distribution parameters in diabetic neuropathy. Proc Inst Mech Eng H. 2004;218(6):431-43.
- – Hall M, Shurr DG, Zimmerman MB, Saltzman CL. Plantar foot surface temperatures with use of insoles. Iowa Orthop J. 2004;24:72-5.
- – Coughlin MJ. Hallux valgus. Am Acad Orthop Surg 1997;46:932-66.
- – Inman VT. Hallux Valgus: a review of etiologic factors. Orthop clin north Am 1974;5:59-66.
- – Tehraninasr A, Saeedi H, Forogh B, Bahramizadeh M, Keyhani MR. Effects of insole with toe-separator and night splint on patients with painful hallux valgus: a comparative study. Prosthet Orthot Int. 2008 Mar;32(1):79-83.
- – Goff JD, Crawford R. Diagnosis and treatment of plantar fasciitis. Am Fam Physician. 2011 Sep 15;84(6):676-82.
- – Cohen M, Abdalla RJ, editores. Lesões nos esportes: diagnóstico, prevenção e tratamento. Rio de Janeiro: Revinter, 2003;394-7.
- – Neufeld SK, Cerrato R. Plantar fasciitis: evaluation and treatment. J Am Acad Orthop Surg. 2008 Jun;16(6):338-46.
- – Williams PL. The painful heel.Br J Hosp Med. 1987 Dec;38(6):562-3.
- – Reeder MT, Dick BH, Atkins JK, Pribis AB, Martinez JM. Stress fractures. Current concepts of diagnosis and treatment. Sports Med. 1996 Sep;22(3):198-212.
- – Patel DS, Roth M, Kapil N. Stress fractures: diagnosis, treatment, and prevention. Am Fam Physician. 2011 Jan 1;83(1):39-46.
- – Mattila VM, Sillanpää PJ, Salo T, Laine HJ, Mäenpää H, Pihlajamäki H. Can orthotic insoles prevent lower limb overuse injuries? A randomized-controlled trial of 228 subjects. Scand J Med Sci Sports. 2011 Dec;21(6):804-8.
- – Withnall R, Eastaugh J, Freemantle N. Do shock absorbing insoles in recruits undertaking high levels of physical activity reduce lower limb injury? A randomized controlled trial. J R Soc Med. 2006 Jan;99(1):32-7.
- – Gardner LI Jr, Dziados JE, Jones BH, Brundage JF, Harris JM, Sullivan R, Gill P. Prevention of lower extremity stress fractures: a controlled trial of a shock absorbent insole. Am J Public Health. 1988 Dec;78(12):1563-7.
- – House CM, Dixon SJ, Allsopp AJ. User trial and insulation tests to determine whether shock-absorbing insoles are suitable for use by military recruits during training. Mil Med. 2004 Sep;169(9):741-6.
- – Windle CM, Gregory SM, Dixon SJ. The shock attenuation characteristics of four different insoles when worn in a military boot during running and marching. Gait Posture. 1999 Mar;9(1):31-7.
- – Jahss MH. The Sesamoids of the Hallux.Current Orthopaedic Practice. 1981:157:88-97
- – Vanore JV, Christensen JC, Kravitz SR, Schuberth JM, Thomas JL, Weil LS, Zlotoff HJ, Couture SD. Diagnosis and treatment od first metatarsophalangeal joint disorders section 4: sesamóide disorders.Clin Pract Guid.2003:42:143-147.
- – Leventen EO. Sesamoid disorders and treatment. An update. Clin Orthop Relat Res. 1991 Aug;(269):236-40.
- – Ferrari R. A cohort-controlled trial of the addition of customized foot orthotics to standard care in fibromyalgia. Clin Rheumatol. 2012 Jul;31(7):1041-5.
- – Maki BE, Sibley KM, Jaglal SB, Bayley M, Brooks D, Fernie GR, Flint AJ, Gage W, Liu BA, McIlroy WE, Mihailidis A, Perry SD, Popovic MR, Pratt J, Zettel JL. Reducing fall risk by improving balance control: development, evaluation and knowledge-translation of new approaches. J Safety Res. 2011 Dec;42(6):473-85.
- – Hossain M, Alexander P, Burls A, Jobanputra P. Foot orthoses for patellofemoral pain in adults. Cochrane Database Syst Rev. 2011 Jan 19;(1)
- – Paton J, Bruce G, Jones R, Stenhouse E. Effectiveness of insoles used for the prevention of ulceration in the neuropathic diabetic foot: a systematic review. J Diabetes Complications. 2011 Jan-Feb;25(1):52-62.
- – Cavanagh PR, Owings TM. Nonsurgical strategies for healing and preventing recurrence of diabetic foot ulcers. Foot Ankle Clin. 2006 Dec;11(4):735-43.
- – Inlow S, Kalla TP, Rahman J. Downloading plantar foot pressures in the diabetic patient. Ostomy Wound Manage. 1999 Oct;45(10):28-34, 36, 38 quiz 39-40.
- – Abu-Faraj ZO, Harris GF, Chang AH, Shereff MJ. Evaluation of a rehabilitative pedorthic: plantar pressure alterations with scaphoid pad application. IEEE Trans Rehabil Eng. 1996 Dec;4(4):328-36.
- – Janisse DJ. Prescription insoles and footwear. Clin Podiatr Med Surg. 1995 Jan;12(1):41-61.
- – Anderson EG. Fatigue fractures of the foot. Injury. 1990 Sep;21(5):275-9.
- – McKeon PO, Stein AJ, Ingersoll CD, Hertel J. Altered plantar-receptor stimulation impairs postural control in those with chronic ankle instability. J Sport Rehabil. 2012 Feb;21(1):1-6.
- – Alcacer-Pitarch B, Buch MH, Gray J, Denton CP, Herrick A, Navarro-Coy N, Collier H, Loughrey L, Pavitt S, Siddle HJ, Wright J, Helliwell PS, Emery P, Redmond AC. Pressure and pain in systemic sclerosis/scleroderma–an evaluation of a simple intervention (PISCES): randomised controlled trial protocol. BMC Musculoskelet Disord. 2012 Feb 6;13:11.
- – Turpin KM, De Vincenzo A, Apps AM, Cooney T, MacKenzie MD, Chang R, Hunt MA.Biomechanical and clinical outcomes with shock-absorbing insoles in patients with knee osteoarthritis: immediate effects and changes after 1 month of wear. Arch Phys Med Rehabil. 2012 Mar;93(3):503-8.
- – Fantini Pagani CH, Hinrichs M, Brüggemann GP. Kinetic and kinematic changes with the use of valgus knee brace and lateral wedge insoles in patients with medial knee osteoarthritis.J Orthop Res. 2012 Jul;30(7):1125-32.
- – Shih YF, Wen YK, Chen WY. Application of wedged foot orthosis effectively reduces pain in runners with pronated foot: a randomized clinical study. Clin Rehabil. 2011 Oct;25(10):913-23.
- – Kutzner I, Damm P, Heinlein B, Dymke J, Graichen F, Bergmann G. The effect of laterally wedged shoes on the loading of the medial knee compartment-in vivo measurements with instrumented knee implants. J Orthop Res. 2011 Dec;29(12):1910-5.
- – Sungkarat S, Fisher BE, Kovindha A. Efficacy of an insole shoe wedge and augmented pressure sensor for gait training in individuals with stroke: a randomized controlled trial. Clin Rehabil. 2011 Apr;25(4):360-9.
- – Perhamre S, Lundin F, Norlin R, Klässbo M. Sever’s injury; treat it with a heel cup: a randomized, crossover study with two insole alternatives. Scand J Med Sci Sports. 2011 Dec;21(6):e42-7.
- – Hartmann A, Murer K, de Bie RA, de Bruin ED. The effect of a training program combined with augmented afferent feedback from the feet using shoe insoles on gait performance and muscle power in older adults: a randomised controlled trial. Disabil Rehabil. 2010;32(9):755-64.
- – Hinman RS, Bowles KA, Bennell KL. Laterally wedged insoles in knee osteoarthritis: do biomechanical effects decline after one month of wear? BMC Musculoskelet Disord. 2009 Nov 25;10:146.
- – Segal NA, Foster NA, Dhamani S, Ohashi K, Yack HJ. Effects of concurrent use of an ankle support with a laterally wedged insole for medial knee osteoarthritis. PM R. 2009 Mar;1(3):214-22.
- – Cho NS, Hwang JH, Chang HJ, Koh EM, Park HS. Randomized controlled trial for clinical effects of varying types of insoles combined with specialized shoes in patients with rheumatoid arthritis of the foot. Clin Rehabil. 2009 Jun;23(6):512-21.
- – Nakajima K, Kakihana W, Nakagawa T, Mitomi H, Hikita A, Suzuki R, Akai M, Iwaya T, Nakamura K, Fukui N. Addition of an arch support improves the biomechanical effect of a laterally wedged insole. Gait Posture. 2009 Feb;29(2):208-13.
- – Ki SW, Leung AK, Li AN. Comparison of plantar pressure distribution patterns between foot orthoses provided by the CAD-CAM and foam impression methods. Prosthet Orthot Int. 2008 Sep;32(3):356-62.
- – Perry SD, Radtke A, McIlroy WE, Fernie GR, Maki BE. Efficacy and effectiveness of a balance-enhancing insole. J Gerontol A Biol Sci Med Sci. 2008 Jun;63(6):595-602.
- – Rodrigues PT, Ferreira AF, Pereira RM, Bonfá E, Borba EF, Fuller R. Effectiveness of medial-wedge insole treatment for valgus knee osteoarthritis. Arthritis Rheum. 2008 May 15;59(5):603-8.
- – O’Leary K, Vorpahl KA, Heiderscheit B. Effect of cushioned insoles on impact forces during running. J Am Podiatr Med Assoc. 2008 Jan-Feb;98(1):36-41.
- – Toda Y, Tsukimura N. A 2-year follow-up of a study to compare the efficacy of lateral wedged insoles with subtalar strapping and in-shoe lateral wedged insoles in patients with varus deformity osteoarthritis of the knee. Osteoarthritis Cartilage. 2006 Mar;14(3):231-7. Epub 2005 Nov 3.
- – Toda Y, Tsukimura N, Segal N. An optimal duration of daily wear for an insole with subtalar strapping in patients with varus deformity osteoarthritis of the knee. Osteoarthritis Cartilage. 2005 Apr;13(4):353-60.
- – Toda Y, Tsukimura N. A six-month followup of a randomized trial comparing the efficacy of a lateral-wedge insole with subtalar strapping and an in-shoe lateral-wedge insole in patients with varus deformity osteoarthritis of the knee. Arthritis Rheum. 2004 Oct;50(10):3129-36.
- – Toda Y, Tsukimura N, Kato A. The effects of different elevations of laterally wedged insoles with subtalar strapping on medial compartment osteoarthritis of the knee. Arch Phys Med Rehabil. 2004 Apr;85(4):673-7.
- – Toda Y, Segal N. Usefulness of an insole with subtalar strapping for analgesia in patients with medial compartment osteoarthritis of the knee. Arthritis Rheum. 2002 Oct 15;47(5):468-73.
- – Toda Y, Segal N, Kato A, Yamamoto S, Irie M. Correlation between body composition and efficacy of lateral wedged insoles for medial compartment osteoarthritis of the knee. J Rheumatol. 2002 Mar;29(3):541-5
- – Toda Y, Segal N, Kato A, Yamamoto S, Irie M. Correlation between body composition and efficacy of lateral wedged insoles for medial compartment osteoarthritis of the knee. J Rheumatol. 2002 Mar;29(3):541-5
- – Kuroyanagi Y, Nagura T, Matsumoto H, Otani T, Suda Y, Nakamura T, Toyama Y. The lateral wedged insole with subtalar strapping significantly reduces dynamic knee load in the medial compartment gait analysis on patients with medial knee osteoarthritis. Osteoarthritis Cartilage. 2007 Aug;15(8):932-6.
- – Ciuffolo F, Ferritto AL, Muratore F, Tecco S, Testa M, D’Attilio M, Festa F. Immediate effects of plantar inputs on the upper half muscles and upright posture: a preliminary study. Cranio. 2006 Jan;24(1):50-9.
- – Branthwaite HR, Payton CJ, Chockalingam N. The effect of simple insoles on three-dimensional foot motion during normal walking. Clin Biomech (Bristol, Avon). 2004 Nov;19(9):972-7.
- – Waddington G, Adams R. Football boot insoles and sensitivity to extent of ankle inversion movement. Br J Sports Med. 2003 Apr;37(2):170-4; discussion 175.
- – Gillespie KA, Dickey JP. Determination of the effectiveness of materials in attenuating high frequency shock during gait using filterbank analysis. Clin Biomech (Bristol, Avon). 2003 Jan;18(1):50-9.
- – House CM, Waterworth C, Allsopp AJ, Dixon SJ. The influence of simulated wear upon the ability of insoles to reduce peak pressures during running when wearing military boots. Gait Posture. 2002 Dec;16(3):297-303.
- – Ogon M, Aleksiev AR, Spratt KF, Pope MH, Saltzman CL. Footwear affects the behavior of low back muscles when jogging. Int J Sports Med. 2001 Aug;22(6):414-9.
- – Redmond A, Lumb PS, Landorf K. Effect of cast and noncast foot orthoses on plantar pressure and force during normal gait. J Am Podiatr Med Assoc. 2000 Oct;90(9):441-9.
- – Uchio Y, Ochi M, Adachi N, Shu N. Effectiveness of an insole with a lateral wedge for idiopathic osteonecrosis of the knee. J Bone Joint Surg Br. 2000 Jul;82(5):724-7.
- – Crenshaw SJ, Pollo FE, Calton EF. Effects of lateral-wedged insoles on kinetics at the knee. Clin Orthop Relat Res. 2000 Jun;(375):185-92.
- – Randolph AL, Nelson M, deAraujo MP, Perez-Millan R, Wynn TT. Use of computerized insole sensor system to evaluate the efficacy of a modified ankle-foot orthosis for redistributing heel pressures. Arch Phys Med Rehabil. 1999 Jul;80(7):801-4.
- – Kästenbauer T, Sokol G, Auinger M, Irsigler K. Running shoes for relief of plantar pressure in diabetic patients. Diabet Med. 1998 Jun;15(6):518-22.
- – Reiber GE, Smith DG, Boone DA, del Aguila M, Borchers RE, Mathews D, Joseph AW, Burgess EM. Design and pilot testing of the DVA/Seattle Footwear System for diabetic patients with foot insensitivity. J Rehabil Res Dev. 1997 Jan;34(1):1-8.
- – Caselli MA, Levitz SJ, Clark N, Lazarus S, Velez Z, Venegas L. Comparison of Viscoped and PORON for painful submetatarsal hyperkeratotic lesions. J Am Podiatr Med Assoc. 1997 Jan;87(1):6-10.
- – Seboka G, Alert PS. Cost-effective footwear for leprosy control programmes: a study in rural Ethiopia. Lepr Rev. 1996 Sep;67(3):208-16.
- – Nawoczenski DA, Janisse DJ. Foot orthoses in rehabilitation – what’s new. Clin Sports Med. (2004) 23:157-167.
- – Nawoczenski DA, Ludewig PM. Electromyographic effects of foot orthotics on selected lower extremity muscles during running. Arch Phys Med Rehabil 1999;80(5):540– 4.
- – Picon AP, Ortega NRS, Watari R, Sartor C, Sacco ICN. Classification of the severity of diabetic neuropathy: a new approach taking uncertainties into account using fuzzy logic. Clinics 2012;67(2):151-156.
- – Mann RA, Coughlin. Hallux valgus- etiology, anatomy, treatment and surgical considerations. Clin orthop 1981;157:31-41.
- – Reynolds JC. Developmental disorders: adult foot part 2. Metatarsalgia. The foot Book. Gould-Baltimore: Wiliams & Wilkins 1988:219-227.
- – Civinni F. Su di un gangliare rigonfiamento della piñata del piede.Mem Chir Archiespedale Pistoia.1835:4–17.
- – Durlacher L.A treeatise on corns, bunions, the disease of nails, and the generalmanagement of the feet. London: Simpkin, Marshall; 1845. p. 52.
- – Oishi A, Prior M, Worley A. The use of foot orthoses in the management of rheumatoid arthritis patient. The internet journal of allied health sciences and practice; 2011.
Anexo 2: Sobre os Autores:

Ulisses Taddei é fisioterapeuta formado pela Faculdade de Medicina da Universidade de São Paulo (USP) e especialista em Reeducação Funcional da Postura e do Movimento pelo Hospital das Clínicas de São Paulo (HC-FMUSP). Realizou pesquisas e publicou artigos em biomecânica e antropometria em revistas científicas internacionais junto a importantes pesquisadores da área. Atualmente é responsável pelos projetos e desenhos de órteses na empresa Pés Sem Dor.
Thomas Amos Case, PhD é engenheiro mecânico pela Michigan State University, MBA pela Oklahoma City University e PhD em negócios internacionais pela The University of Michigan. É fundador e consultor da empresa Pés Sem Dor.

Cristian Vilela dos Santos é médico formado pela Faculdade de Medicina da Universidade de São Paulo (USP), especialista em tornozelo e pé pelo instituto de ortopedia e traumatologia (IOT/HC-FMUSP), membro da sociedade Brasileira de Ortopedia e Traumatologia e chefe do pronto-atendimento da Eq. Prof. Dr. Alberto T. Croci do hospital Beneficência Portuguesa de São Paulo.
Anexo 3: Abstracts
Resumos relacionados à Diabetes:
J Diabetes Complications. 2011 Jan-Feb;25(1):52-62. doi: 10.1016/j.jdiacomp.2009.09.002. Epub 2009 Oct 23.
Effectiveness of insoles used for the prevention of ulceration in the neuropathic diabetic foot: a systematic review.
Paton J, Bruce G, Jones R, Stenhouse E.
Source
University of Plymouth, Plymouth, Devon, UK. joanne.paton@plymouth.ac.uk
Abstract
CONTEXT:
Ulceration can be a debilitating and costly complication of the neuropathic diabetic foot. Insoles inserted into footwear are routinely used in clinical practice to help to prevent ulceration. AIM AND SCOPE OF THE REVIEW: This review evaluated the effectiveness of insoles used for the prevention of ulcer in the neuropathic diabetic foot.
METHODS:
Databases were searched from inception to 2008, supplemented by hand searching of references and grey literature. Data extraction and methodological quality assessment were independently conducted by two reviewers following the recommendations of the Centre for Reviews and Dissemination.
RESULTS:
A total of five trials met the inclusion criteria: two randomised control trials (RCTs), two case control studies, and one follow-up study. The methodological quality of the majority of studies was poor. Omitted details regarding the generalisability of results made study comparison and inference to practice difficult. There is a small amount of limited evidence indicating that insoles are effective in reducing incidence of ulceration and reducing plantar peak pressures in the diabetic neuropathic foot. No study included economic analysis or patient-based outcome measures.
CONCLUSIONS:
Insoles appear of use for the prevention of neuropathic diabetic foot ulceration, although evidence is limited. Clinical recommendation regarding type and specification of insole is not possible at this time. There is an essential need for a large well-designed RCT comparing different types of commonly used insole for the prevention of ulceration in the diabetic neuropathic foot. Outcome measures should include patient perceptions of the effectiveness and cost-effectiveness analysis.
Foot Ankle Clin. 2006 Dec;11(4):735-43.
Nonsurgical strategies for healing and preventing recurrence of diabetic foot ulcers.
Source
Department of Biomedical Engineering, Lerner Research Institute, Cleveland Clinic, 9500 Euclid Ave., Cleveland, OH 44195, USA. cavanagh@ccf.org
Abstract
We have outlined an approach to the nonsurgical treatment of diabetic foot ulcers based on an understanding of their etiology. We have emphasized the importance of off-loading as the crucial element to success in healing foot ulcers and preventing their recurrence in those with diabetes. Computerized design of custom insoles can allow the unloading of elevated plantar pressure while incorporating the shape of the foot, which was formerly the major criterion used insole design.
Ostomy Wound Manage. 1999 Oct;45(10):28-34, 36, 38 quiz 39-40.
Downloading plantar foot pressures in the diabetic patient.
Source
Calgary Foot Care Clinic, Alberta, Canada.
Abstract
Pressure downloading (offloading) is the most important component in the prevention and treatment of diabetic foot ulcers because peripheral neuropathy is a major contributing factor to more than 90% of all diabetic foot ulcers. Downloading techniques range from the simplest insole, through many types of orthotics and footwear modifications including the ankle-foot orthosis and total contact casting, to surgical procedures. A philosophical difference exists between surgical and nonsurgical approaches, with the patient subjected to the bias of the practitioner. This article explores uniting both surgical and nonsurgical pressure downloading techniques, using a modified Carville Classification System to help the practitioner determine the appropriate method(s) of downloading. By adding a Category 4 to include diabetic persons with foot ulcers or acute Charcot events, a seamless system is obtained to categorize and treat all people with diabetes with pressure downloading recommendations.
Clin Podiatr Med Surg. 1995 Jan;12(1):41-61.
Prescription insoles and footwear.
Source
National Pedorthic Services, Inc, Milwaukee, Wisconsin, USA.
Abstract
Current research emphasizes the importance of prevention in caring for the diabetic foot. Prescription footwear has been shown to be a significant factor in prevention of both ulcer recurrence and amputation. In addition, scientific evidence demonstrates the ability of insole materials to reduce shock and shear, the effectiveness of insoles in providing pressure relief, and the ability of rocker soles to relieve metatarsal pressure. This evidence, however, is limited and is often based on clinical investigation rather than on objective, quantitative measurements. Recent advances in biomechanical modeling and in-shoe pressure measurement should allow more objective data on a wider variety of prescription footwear to become available. The importance of prescription footwear as a preventive measure is nonetheless widely recognized. The knowledge and experience of pedorthists make them uniquely qualified to provide the needed shoes, modifications, and insoles for the long-term management of the diabetic foot.
Diabetes Care. 2011 Jul;34(7):1595-600. doi: 10.2337/dc10-2206. Epub 2011 May 24.
Evaluation and optimization of therapeutic footwear for neuropathic diabetic foot patients using in-shoe plantar pressure analysis.
Bus SA, Haspels R, Busch-Westbroek TE.
Source
Department of Rehabilitation, Academic Medical Center, University of Amsterdam, Amsterdam, the Netherlands. s.a.bus@amc.uva.nl
Abstract
OBJECTIVE:
Therapeutic footwear for diabetic foot patients aims to reduce the risk of ulceration by relieving mechanical pressure on the foot. However, footwear efficacy is generally not assessed in clinical practice. The purpose of this study was to assess the value of in-shoe plantar pressure analysis to evaluate and optimize the pressure-reducing effects of diabetic therapeutic footwear.
RESEARCH DESIGN AND METHODS:
Dynamic in-shoe plantar pressure distribution was measured in 23 neuropathic diabetic foot patients wearing fully customized footwear. Regions of interest (with peak pressure>200 kPa) were selected and targeted for pressure optimization by modifying the shoe or insole. After each of a maximum of three rounds of modifications, the effect on in-shoe plantar pressure was measured. Successful optimization was achieved with a peak pressure reduction of >25% (criterion A) or below an absolute level of 200 kPa (criterion B).
RESULTS:
In 35 defined regions, mean peak pressure was significantly reduced from 303 (SD 77) to 208 (46) kPa after an average 1.6 rounds of footwear modifications (P<0.001). This result constitutes a 30.2% pressure relief (range 18-50% across regions). All regions were successfully optimized: 16 according to criterion A, 7 to criterion B, and 12 to criterion A and B. Footwear optimization lasted on average 53 min.
CONCLUSIONS:
These findings suggest that in-shoe plantar pressure analysis is an effective and efficient tool to evaluate and guide footwear modifications that significantly reduce pressure in the neuropathic diabetic foot. This result provides an objective approach to instantly improve footwear quality, which should reduce the risk for pressure-related plantar foot ulcers.
Prosthet Orthot Int. 2007 Sep;31(3):228-35.
Effect of flat insoles with different Shore A values on posture stability in diabetic neuropath.
Van Geffen JA, Dijkstra PU, Hof AL, Halbertsma JP, Postema K.
Source
Center for Rehabilitation, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands. H.v.Geffen@grootklimmendaal.nl
Abstract
The objective of the study was to determine whether insoles with a low Shore A value (15 degrees) as prescribed for patients with a diabeticneuropathy have a negative effect on posture stability because these insoles may reduce somatosensory input under the feet. It was conducted in the Center for Rehabilitation, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands The study was observational and conducted on 30 diabetic patients (aged 37 – 82 years) with a neuropathy. Posture stability (body sway) was assessed in a shoe without insole, on aflat insole with a low Shore A value (15 degrees) and on a flat insole with a higher Shore A value (30 degrees). These assessments were done under four different conditions: (1) eyes open, no dual-task, (2) eyes closed, no dual-task, (3) eyes open, dual-task (mental arithmetic) and (4) eyes closed, dual-task. Additionally 10 healthy controls (aged 27 – 51 years) were assessed similarly. A significantly higher root-mean-square (rms) value of the anterior-posterior velocity, V(y), was found in patients compared with controls (3.4 cm/s vs. 1.2 cm/s, p < 0.05). Also a significant difference in rms value of the anterior-posterior velocity, V(y), was found between eyes open and eyes closed (1.9 cm/s vs. 2.7 cm/s, p < 0.05). No significant effects were found for insoles or dual tasks for the total group. In diabetic patients no significant effect was found of insoles on posture stability. The effect of closed eyes on posture stability was significantly larger for diabetic patients compared to controls. It was found that prescribing insoles with a lowShore A value (15 degrees), compared to insoles with a higher Shore A value (30 degrees) has no significant negative effect on posture stability in patients with a diabetic neuropathy.
Proc Inst Mech Eng H. 2004;218(6):431-43.
Effect of foot sole hardness, thickness and footwear on foot pressure distribution parameters in diabetic neuropathy.
Charanya G, Patil KM, Narayanamurthy VB, Parivalavan R, Visvanathan K.
Source
Biomedical Engineering Division, Department of Applied Mechanics, Indian Institute of Technology, Chennai, Madras-600036, India.
Abstract
This paper presents details of the study undertaken to find the effects of foot sole hardness, thickness and footwear on walking-foot pressure distribution parameters (power ratio (PR)) in diabetic neuropathy. The foot sole hardness is characterized by Shore level. PR represents the ratio of high-frequency power to the total power in the power spectrum of the walking-foot pressure image distribution obtained from the optical pedobarograph. Spatial frequency distributions in the walking-foot pressure images were analysed to calculate the PR in each of the foot sole areas at different levels of foot sole sensation loss and mechanical and geometrical properties. The results show that the increase in PR in the upper foot sole Shore ranges (30-40) is 1.2-2.5 times the corresponding increase in lower Shore ranges (20-30) for some foot sole areas, implying a higher possibility of development of plantar ulcers when combined with deterioration of foot sole sensation. Plantar ulcers are found in feet with foot sole Shore values of 30, a sensation level of 45 mN and PR of 35; for Shore values of 40, sensation levels of 100 mN, with PR 52; and for Shore values above 40, sensation level > 100 mN with PR 58. Providing microcellular rubber insole footwear based on optimum hardness and thickness was found to be helpful in healing plantar ulcers in three to four weeks. Wearing preventive footwear for six months reduced hardness of the foot sole and PR values to near-normal values.
Iowa Orthop J. 2004;24:72-5.
Plantar foot surface temperatures with use of insoles.
Hall M, Shurr DG, Zimmerman MB, Saltzman CL.
Source
Orthopaedics and Rehabilitation Bioengineering, University of Iowa, IA, USA.
Abstract
PURPOSE:
Patients with diabetes are often prescribed foot orthoses to help prevent foot ulcer formation. Orthotics are used to redistribute normal and shear stress. Shear stresses are not easily measurable and considered to be responsible for skin breakdown. Local elevation of skin temperature has been implicated as an early sign of impending ulceration especially in regions of high shear stress. The purpose of this study was to measure the effects of commonly prescribed insole materials on local changes in plantar foot temperature during normal gait.
METHODS:
Six commonly used foot orthosis materials were tested using the Thermo Trace infrared thermometer to measure foot temperature. Ten healthy adult volunteers without any history of diabetes or abnormal sensation participated in the study. During each trial the subject walked on a treadmill with the test material in the dominant foot’s shoe, for six minutes at a speed of four miles per hour and rested for six minutes between trials. Four locations on the foot (hallux, first and fifth metatarsal heads, and heel) and the contralateral bicep temperatures were measured at 0, 1, 3, 5 minutes during the rest period. The order of material and skin location testing was randomized.
RESULTS:
Significant differences were found between baseline temperatures and foot temperatures for all materials. However, no differences were found between materials for any location on the foot.
CONCLUSION:
Previous studies have attempted to characterize materials based on laboratory and clinical testing, while other studies have attempted to characterize the effect of pressure on skin temperature. However, no study has previously attempted to characterize foot orthosis materials based on foot temperatures. This study compared foot temperatures of healthy adults based on the material tested. Although this study was unable to distinguish between materials based on foot temperatures, it was able to show a rise in foot temperature with any material used. This study demonstrates a need to a larger study on a population with diabetes.
Clin Biomech (Bristol, Avon). 2004 Jul;19(6):629-38.
Pressure relief and load redistribution by custom-made insoles in diabetic patients with neuropathy and footdeformity.
Bus SA, Ulbrecht JS, Cavanagh PR.
Source
Department of Internal Medicine, Academic Medical Center, University of Amsterdam, 1100 DE Amsterdam, The Netherlands.
Abstract
OBJECTIVE:
To study the effects of custom-made insoles on plantar pressures and load redistribution in neuropathic diabetic patients with footdeformity.
DESIGN:
Cross-sectional.
BACKGROUND:
Although custom-made insoles are commonly prescribed to diabetic patients, little quantitative data on their mechanical action exists.
METHODS:
Regional in-shoe peak pressures and force-time integrals were measured during walking in the feet of 20 neuropathic diabetic subjects with foot deformity who wore flat or custom-made insoles. Twenty-one feet with elevated risk for ulceration at the first metatarsal head were analysed.Load redistribution resulting from custom-made insoles was assessed using a new load-transfer algorithm.
RESULTS:
Custom-made insoles significantly reduced peak pressures and force-time integrals in the heel and first metatarsal head regions; pressures and integrals were significantly increased in the medial midfoot region compared with flat insoles. Custom-made insoles successfully reduced pressures in and integrals at the first metatarsal head in 7/21 feet, were moderately successful in another seven, but failed in the remaining seven. Load transfer was greatest from the lateral heel to the medial midfoot regions.
CONCLUSIONS:
Custom-made insoles were more effective than flat insoles in off-loading the first metatarsal head region, but with considerable variability between individuals. Most off-loading occurred in the heel (not a region typically at risk). The load transfer algorithm effectively analysescustom-made-insole action.
RELEVANCE:
Because similar insole modifications apparently exert different effects in different patients, a comprehensive evaluation of custom designs using in-shoe pressure measurement should ideally be conducted before dispensing insoles to diabetic patients with neuropathy and footdeformity.
Diabet Med. 2001 Apr;18(4):314-9.
Effects of preventative footwear on foot pressure as determined by pedobarography in diabetic patients: aprospective study.
Lobmann R, Kayser R, Kasten G, Kasten U, Kluge K, Neumann W, Lehnert H.
Source
Department of Endocrinology and Metabolism, University Medical School of Magdeburg, Germany.
Abstract
AIMS:
This study analysed the effects of specially manufactured insoles on foot pressures in diabetic patients during a 1-year prospective observation period.
METHODS:
We studied 81 type 2 diabetic patients without foot lesions. Using pedobarography three different regions of interest were examined: maximum peak pressure (MPP) of the total foot area, heel region and head of metatarsal bone I-III. Eighteen patients with high risk pressure (MPP of total foot 474 +/- 183 kPa; heel region 278 +/- 147 kPa, metatarsal 389 +/- 222 kPa) received optimal insole support. Sixty-three patients as a control group (MMP of total foot 367.7 +/- 157 kPa; heel 263.1 +/- 127 kPa, metatarsal 339.9 +/- 171 kPa) received conventional footwear.
RESULTS:
After insole support a 30% pressure reduction of total foot MMP (474 +/- 183 kPa vs. 290 +/- 106 kPa) was achieved in the treatment group. After 6 months (324 +/- 127 kPa) and 1 year (380 +/- 190 kPa) a pressure reduction was found. Between the 6- and 12-month controls plantar pressures again increased. In the control group a significant increase of all peak pressures occurred.
CONCLUSIONS:
Early insole support is successful in reducing plantar pressure. A repeated adjustment should be performed every 6 months to prevent foot pressure increases. The comparison of foot pressure development between the two groups showed constant levels in the treatment group. In the control group a marked increase of the pressure values was found. Identification and subsequent support of patients with high ulceration risk may help to reduce the high amputation rate.
Diabetes Care. 2000 Dec;23(12):1746-51.
Effectiveness and safety of a nonremovable fiberglass off-bearing cast versus a therapeutic shoe in the treatment of neuropathic foot ulcers: a randomized study.
Caravaggi C, Faglia E, De Giglio R, Mantero M, Quarantiello A, Sommariva E, Gino M, Pritelli C, Morabito A.
Source
Center for the Study and Treatment of Diabetic Foot Pathology, Ospedale di Abbiategrasso, Sesto S. Giovanni, Milan, Italy. cara@mail3.telnetwork.it
Abstract
OBJECTIVE:
To evaluate and compare the rate of reduction of the surface area of neuropathic plantar ulcers in diabetic patients treated with nonremovable rigidity-differentiated fiberglass off-bearing casts or a cloth shoe with a rigid sole with unloading alkaform insoles. The secondary aim was to evaluate the side effects and degree of patient acceptance of treatment.
RESEARCH DESIGN AND METHODS:
Fifty diabetic patients with neuropathic plantar ulcers were consecutively enrolled and randomized to one of two treatment groups. Of the 50 patients, 24 were treated with a specialized cloth shoe with a rigid sole and an unloading alkaform insole (shoe group), and 26 patients were treated with a nonremovable off-bearing fiberglass cast (cast group). All patients in both study groups returned to the clinic for weekly control visits. Their ulcers were treated with a standard dressing. Tracings of the ulcer area using a transparent dressing were performed on the day of entry to the study and after 30 days of treatment. The presence of new ulcerations caused by the use of the pressure-relief apparatus was recorded. Patient acceptance of the treatment was measured using a visual analog scale.
RESULTS:
At the end of the treatment period, an 8.3% increase of the ulcer area was observed in two patients in the shoe group, whereas in the cast group, no patient presented an increase. The reduction of the ulcer area was statistically more rapid in the cast group (Mann-Whitney test, P = 0.0004). Furthermore, the number of ulcers completely healed at the 30-day time point was 13 (50%) in the cast group and 5 (20.8%) in the shoe group (P = 0.03). In both groups, no side effects were recorded. The average score +/- SD of patient acceptance was 91.15 +/- 9.9 in the shoe group and 88.33 +/- 17.3 (NS) in the cast group.
CONCLUSIONS:
Our study has shown a significant difference in the speed of the reduction of neuropathic plantar ulcers treated with a fiberglass cast compared with a specialized cloth shoe. The use of fiberglass material with variable rigidity has also shown two important results: the elimination of side effects including ulcers caused by the cast, and high patient acceptance. These data show that the use of off-bearing casts made with fiberglass bandages of variable rigidity is the elective treatment of neuropathic plantar ulcers.
Diabet Med. 1998 Jun;15(6):518-22.
Running shoes for relief of plantar pressure in diabetic patients.
Kästenbauer T, Sokol G, Auinger M, Irsigler K.
Source
- Boltzmann Research Institute for Metabolic Diseases and Nutrition, Vienna-Lainz Hospital, Vienna, Austria.
Abstract
There is a causal relationship between diabetic foot ulceration, elevated plantar pressure, and severe sensory neuropathy. Cushioned footwear intended to relieve plantar pressure is well established for prevention and healing of plantar ulcers. The aim of the present study was to investigate whether pressure relief by means of a running shoe with optimized forefoot pressure damping is comparable to that of a custom-made soft insole placed into an in-depth shoe. The in-shoe pressures were compared to an in-depth shoe with the original cork insole and with a leather-soled Oxford shoe. The maximum reduction of plantar pressure in the running shoe was 47% under the 2nd and 3rd metatarsal heads, 29% at the first metatarsal head, and 32% at the great toe in comparison to the Oxford shoe. This was surpassed only by the custom-made insole, which reduced pressures at the metatarsal heads by 50%. The specially designed running shoe yielded the same pressure relief at the central metatarsal heads as the custom-made insole. Such shoes are likely to be very useful in preventing diabetic foot ulceration in high-risk patients as a comparatively affordable and immediately available device.
J Rehabil Res Dev. 1997 Jan;34(1):1-8.
Design and pilot testing of the DVA/Seattle Footwear System for diabetic patients with foot insensitivity.
Reiber GE, Smith DG, Boone DA, del Aguila M, Borchers RE, Mathews D, Joseph AW, Burgess EM.
Source
Prosthetics Research Study, Seattle, WA 98122, USA.
Abstract
Clinical epidemiology studies suggest the majority of lower limb amputations were preceded by a minor traumatic event, often footwear-related, and lower limb ulcers. To reduce foot trauma and ulcers, the diabetic patient with foot insensitivity has unique footwear needs. To address these needs forpatients not requiring custom shoes, the DVA/Seattle Footwear System was developed. The six components of this system include: 1) a specially designed shoe last based on the geometry of the diabetic foot and research findings on foot regions at highest risk of ulceration, 2) a depth-inlay shoe, “Custom Stride by PRS,” designed to be paired with either a custom-fabricated cork insole or a preformed polyurethane insole, 3) a laser digitizing system that captures 3-D plantar foot contours, 4) DVA/Seattle ShapeMaker software adaptation for modifying plantar surface contours and applying free-form and template modifications to increase or relieve loading, 5) software that translates files into code used by a milling machine to define the cutting path and carve cork blockers into custom insoles, and 6) a preformed polyurethane insole thicker than a typical insole to accommodate the extra volume and the interior dimensions of the shoe. A 6-month pilot cross-over trial of 24 diabetic male veterans without prior footulcers was conducted to determine the feasibility of producing, and the safety of wearing, these depthinlay shoes and both types of insoles. During the first 4 weeks, patients were assigned to the study shoes and one type of insole. During the next 4 weeks, they wore the other type of insole, and during the final 4 months, they chose which pair of insoles to wear with the study shoes. Over 150 person-months of footwear observation revealed no breaks in the cutaneous barrier with use of either cork or polyurethane insoles and the study shoes. Patient compliance with the footwear was 88%.Patients were highly satisfied with the appearance, stability, and comfort of the shoes and the comfort of both types of insole. However, 75% of thepatients noted that the study shoes felt heavier than their customary shoes. Further research is needed to determine the long-term effectiveness offootwear in prevention of foot ulcers in the population at highest risk for diabetic reulceration and amputation.
Resumos associados a Osteoartrite:
Ann Readapt Med Phys. 2005 Dec;48(9):682-9. Epub 2005 Jun 13.
[Feet insoles and knee osteoarthritis: evaluation of biomechanical and clinical effects from a literature review].
Gélis A, Coudeyre E, Aboukrat P, Cros P, Hérisson C, Pélissier J.
Source
Service central de rééducation fonctionnelle, université Montpellier-I, CHU Lapeyronie, avenue du Doyen-Giraud, 34295 Montpellier, cedex 05, France.
Abstract
OBJECTIVE:
To determine the biomechanical and clinical effectiveness of foot insoles in patients with knee osteoarthritis.
MATERIALS AND METHODS:
A systematic review of the literature (Medline, Pascal and Embase) using the MESH words knee, and insole and plantar orthosis for the biomechanical part and osteoarthritis, and insole and plantar orthosis for the clinical part. Clinical studies were classified by 2 independent readers using the Jadad scale.
RESULTS:
Two biomechanical theories were found: the adduction moment theory, which explains the effect of heel wedging, and articular chain theory, which explains the effect of lateral wedged insoles. The clinical effect was explained more by an anti-algesic effect than an anatomic or functional effect: the treated group consumed fewer nonsteroidal anti-inflammatory drugs than the placebo group for up to 2-years of treatment. Evidence is lacking because of methodological weakness and few clinical trials. The information on side effects is limited.
DISCUSSION:
Laterally wedged foot insoles are proposed for the treatment of knee medial compartment osteoarthritis. The clinical effect is probably limited, but the treatment may reduce the digestive and renal side effects of prolonged use of nonsteroidal anti-inflammatory drugs. Foot insoles could be recommended in clinical practice despite the lack of evidence in comparing the effectiveness of other therapeutics in knee osteoarthritis.
CONCLUSION:
Use of foot insoles is a nonpharmacologic treatment of osteoarthritis of the knee medial compartment.
J Orthop Res. 2012 Jul;30(7):1125-32. doi: 10.1002/jor.22032. Epub 2011 Dec 12.
Braces and orthoses for treating osteoarthritis of the knee.
Brouwer RW, Jakma TS, Verhagen AP, Verhaar JA, Bierma-Zeinstra SM.
Source
Orthopaedic surgery, Erasmus Medical Centre Rotterdam, Dr. Molewaterplein 40, Rotterdam, Netherlands, 3015 GD. r.w.brouwer@mzh.nl
Abstract
BACKGROUND:
Patients with osteoarthritis of the knee can be treated with a brace or orthosis (shoe insole). The main purpose of these aids is to reduce pain, improve physical function and, possibly, to slow disease progression.
OBJECTIVES:
To assess the effectiveness of a brace or orthosis in the treatment of osteoarthritis of the knee.
SEARCH STRATEGY:
We searched Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE and EMBASE (Current contents, Health STAR) up to October 2002. The reference lists of the publications in the identified trials were also screened.
SELECTION CRITERIA:
Extracted studies were included in the final analysis if they met the pre-defined inclusion criteria: 1) a randomised controlled clinical trial or a controlled clinical trial, 2) all patients had osteoarthritis of the knee, 3) the intervention in one of the studied groups was a brace or an orthosis.
DATA COLLECTION AND ANALYSIS:
Two reviewers independently selected the trials and assessed the methodological quality using the Delphi-list and one additional question about care programs. Three reviewers independently extracted the data on the intervention, type of outcome measures, follow-up, loss to follow-up, and results, using a pre-tested standardized form. Study authors were contacted for additional information.
MAIN RESULTS:
Four trials involving a total of 444 people were included in this review. One study investigated a knee brace and three studies examined different types of orthoses for medial compartment osteoarthritis of the knee. Two studies were of high methodological quality while the other two studies were low. Notably, the randomisation and the blinding procedures were either insufficient or not described. The follow-up period (six weeks to six months) was too short to demonstrate long-term results. Pooling was difficult primarily due to the heterogeneity of the data and the way the information was presented. The pain, stiffness and physical function (WOMAC and MACTAR) scores of a brace group showed greater improvement at six months compared with a neoprene sleeve group, which showed greater improvement compared with a control group. The numbers of days of non-steroidal anti-inflammatory drug (NSAID) intake decreased significantly (relative percentage difference 23.9%) compared with baseline in a group with laterally wedged insoles,and remained unchanged in the neutrally wedged group. Patient compliance with the laterally wedged insole was significantly better compared with the neutrally wedged insole. In one study, the Visual Analogue Pain (VAS) pain score was significantly decreased from baseline in a strapped insole group (RPD – 24%), but not in the traditional lateral wedge group, but this strapped insole showed more adverse effects (popliteal pain, low back pain, and foot sole pain) compared with the traditional lateral wedge insole. Pain during bed rest, after getting up, after getting up from seated position and walking distance was significantly improved in a subtalar strapped group compared with baseline, and no improvement was found in a sock type group. No studies were found that assessed the effectiveness of a brace or orthosis to treat lateral compartment osteoarthritis or general osteoarthritis of the knee, or that compared a knee brace with a wedge insole, or that compared a brace or orthosis with operative treatment.
AUTHORS’ CONCLUSIONS:
Based on one brace study we conclude there is limited evidence that: a brace has additional beneficial effect (WOMAC, MACTAR, function tests) for knee osteoarthritis compared with medical treatment alone.(Silver) a sleeve has additional beneficial effect (WOMAC, function tests) for knee osteoarthritis compared with medical treatment alone.(Silver) a brace is more effective (WOMAC, function tests) than a neoprene sleeve.(Silver) Based on 3 orthoses studies, of which 2 were high quality, (n=2) we conclude there is limited evidence that: a laterally wedged insole decreases NSAID intake compared with a neutral insole. (Silver) patient compliance is better in the laterally wedged insole compared with a neutral insole. (Silver) a strapped insole has more adverse effects than a lateral wedge insole. (Silver).
Arch Phys Med Rehabil. 2012 Mar;93(3):503-8. doi: 10.1016/j.apmr.2011.09.019. Epub 2012 Jan 13.
Biomechanical and clinical outcomes with shock-absorbing insoles in patients with knee osteoarthritis: immediate effects and changes after 1 month of wear.
Turpin KM, De Vincenzo A, Apps AM, Cooney T, MacKenzie MD, Chang R, Hunt MA.
Source
Department of Physical Therapy, University of British Columbia, Vancouver, BC, Canada.
Abstract
OBJECTIVES:
To examine the effectiveness of shock-absorbing insoles in the immediate reduction of knee joint load, as well as reductions in knee joint load, pain, and dysfunction after 1 month of wear, in individuals with knee osteoarthritis (OA).
DESIGN:
Pre-post design with participants exposed to 2 conditions (normal footwear, shock-absorbing insoles) with a 1-month follow-up.
SETTING:
University laboratory for testing and general community for intervention.
PARTICIPANTS:
Community-dwelling individuals (N=16; 6 men, 10 women) with medial compartment knee OA.
INTERVENTION:
Participants were provided with sulcus length shock-absorbing insoles to be inserted into their everyday shoes.
MAIN OUTCOME MEASURES:
Primary outcome measures included the peak, early stance peak, and late stance peak external knee adduction moment (KAM); the KAM impulse (positive area under the KAM curve); and peak tibial vertical acceleration. Secondary outcomes included walking pain, the Western Ontario and McMaster Universities Osteoarthritis Index pain subscale and total score, and a timed stair climb task.
RESULTS:
There was a significant reduction in the late stance peak KAM with shock-absorbing insoles (P=.03) during follow-up compared with the baseline test session. No other immediate or longitudinal significant changes (P>.05) in the other KAM parameters or peak tibial acceleration after use of a shock-absorbing insole were observed. However, significant improvements in all measures of pain and function (P<.05) were observed.
CONCLUSIONS:
Shock-absorbing insoles produced significant reductions in self-reported knee joint pain and physical dysfunction with 1 month of wear in patients with knee OA despite no consistent changes in knee joint load. Further research using randomized controlled trials, with larger sample sizes and explorations into long-term use of shock-absorbing insoles and their effect on disease progression, is warranted.
J Orthop Res. 2012 Jul;30(7):1125-32. doi: 10.1002/jor.22032. Epub 2011 Dec 12.
Kinetic and kinematic changes with the use of valgus knee brace and lateral wedge insoles in patients with medial knee osteoarthritis.
Fantini Pagani CH, Hinrichs M, Brüggemann GP.
Source
Institute of Biomechanics and Orthopaedics, German Sport University Cologne, Am Sportpark Müngersdorf 6, 50933 Köln, Germany. c.fantini@dshs-koeln.de
Abstract
The effect of a valgus knee brace and a lateral wedged insole on knee and ankle kinematics and kinetics was evaluated in ten patients with medial knee osteoarthritis (OA). The knee orthosis was tested in two valgus adjustments (4° and 8°), and the laterally wedged insole was fabricated with an inclination of 4°. A motion capture system and force platforms were used for data collection and joint moments were calculated using inverse dynamics. The valgus moment applied by the orthosis was also measured using a strain gauge implemented in the orthosis’ rotational axis. For the second peak knee adduction moment, decreases of 18%, 21%, and 7% were observed between baseline and test conditions for the orthosis in 4° valgus, in 8° valgus, and insole, respectively. Similar decreases were observed for knee lever arm in the frontal plane. Knee adduction angular impulse decreased 14%, 18%, and 7% from baseline to conditions for the orthosis in 4° valgus, in 8° valgus, and insole, respectively. Knee angle in the frontal plane reached a more valgus position during gait using the valgus knee brace. The valgus moment applied by the orthosis with 8° valgus adjustment was 30% higher than with 4° valgus adjustment. The valgus knee orthosis was more effective than the laterally wedged insole in reducing knee adduction moment in patients with medial knee OA.
Clin Orthop Relat Res. 2010 Jul;468(7):1926-32. doi: 10.1007/s11999-010-1274-z. Epub 2010 Feb 23.
Medial knee osteoarthritis treated by insoles or braces: a randomized trial.
van Raaij TM, Reijman M, Brouwer RW, Bierma-Zeinstra SM, Verhaar JA.
Source
Department of Orthopaedics, HS-105, Erasmus University Medical Center, PO Box 2040, 3000 CA, Rotterdam, The Netherlands. t.vanraaij@mac.com
Abstract
BACKGROUND:
There is controversial evidence regarding whether foot orthoses or knee braces improve pain and function or correct malalignment in selected patients with osteoarthritis (OA) of the medial knee compartment. However, insoles are safe and less costly than knee bracing if they relieve pain or improve function.
QUESTIONS/PURPOSES:
We therefore asked whether laterally wedged insoles or valgus braces would reduce pain, enhance functional scores, and correct varus malalignment comparable to knee braces.
PATIENTS AND METHODS:
We prospectively enrolled 91 patients with symptomatic medial compartmental knee OA and randomized to treatment with either a 10-mm laterally wedged insole (index group, n = 45) or a valgus brace (control group, n = 46). All patients were assessed at 6 months. The primary outcome measure was pain severity as measured on a visual analog scale. Secondary outcome measures were knee function score using WOMAC and correction of varus alignment on AP whole-leg radiographs taken with the patient in the standing position. Additionally, we compared the percentage of responders according to the OMERACT-OARSI criteria for both groups.
RESULTS:
We observed no differences in pain or WOMAC scores between the two groups. Neither device achieved correction of knee varus malalignment in the frontal plane. According to the OMERACT-OARSI criteria, 17% of our patients responded to the allocated intervention. Patients in the insole group complied better with their intervention. Although subgroup analysis results should be translated into practice cautiously, we observed a slightly higher percentage of responders for the insole compared with bracing for patients with mild medial OA.
CONCLUSIONS:
Our data suggest a laterally wedged insole may be an alternative to valgus bracing for noninvasively treating symptoms of medial knee OA.
LEVEL OF EVIDENCE:
Level I, therapeutic study. See the Guidelines for Authors for a complete description of level of evidence.
Arthritis Rheum. 2008 May 15;59(5):603-8. doi: 10.1002/art.23560.
Effectiveness of medial-wedge insole treatment for valgus knee osteoarthritis.
Rodrigues PT, Ferreira AF, Pereira RM, Bonfá E, Borba EF, Fuller R.
Source
School of Medicine, University of São Paulo, São Paulo, Brazil.
Abstract
OBJECTIVE:
To assess the efficacy of medial-wedge insoles in valgus knee osteoarthritis (OA).
METHODS:
Thirty consecutive women with valgus-deformity knee OA > or = 8 degrees were randomized into 2 groups: medial insole (insoles with 8-mm medial elevation at the rearfoot [n = 16]) and neutral insole (similar insole without elevation [n = 14]). Both groups also wore ankle supports. A blinded examiner assessed pain on movement, at rest, and at night with a visual analog scale (VAS), the Lequesne index, and Western Ontario and McMaster Universities Osteoarthritis (WOMAC) Index. Femorotibial, talocalcaneal, and talar tilt angles were evaluated at baseline and after 8 weeks of insole use.
RESULTS:
Significant reductions in the medial insole group were observed for pain on movement (mean +/- SD VAS pre- and postintervention 8.1 +/- 1.5 versus 4.2 +/- 2.4; P = 0.001), at rest (5.1 +/- 2.3 versus 2.7 +/- 2.4; P = 0.002), and at night (6.1 +/- 2.7 versus 3.1 +/- 2.1; P = 0.001). In addition, a decrease in Lequesne (14.7 +/- 3.4 versus 9.6 +/- 3.8; P = 0.001) and WOMAC scores (74.1 +/- 14.2 versus 56.1 +/- 14.9; P = 0.001) was observed for the medial insole group. In the neutral insole group, a significant reduction was observed only for night pain (mean +/- SD VAS pre- and postintervention 5.8 +/- 2.4 versus 4.6 +/- 2.4; P = 0.019). An increase in femorotibial angle (169.0 +/- 3.4 versus 170.8 +/- 3.7; P = 0.001) occurred only in the medial insole group. Moreover, the difference in measured femorotibial angles pre- and postintervention was 1.84 +/- 1.42 versus -0.18 +/- 0.67 (P < 0.001) for the medial and neutral insole groups.
CONCLUSION:
The use of medial-wedge insoles was highly effective in reducing pain at rest and on movement and promoted a functional improvement of valgus knee OA.
Osteoarthritis Cartilage. 2008 Feb;16(2):244-53. Epub 2007 Aug 13
Influence of concomitant heeled footwear when wearing a lateral wedged insole for medial compartmentosteoarthritis of the knee.
Source
Toda Orthopedic Rheumatology Clinic, Suita, Osaka, Japan. UGJ72766@nifty.com
Abstract
OBJECTIVE:
To compare the influence of concomitant heeled footwear when wearing a lateral wedged insole for medial compartment of osteoarthritis(OA) of the knee, between everyday walking shoes for outdoor use and socks or flat footwear without a heel for indoor use.
DESIGN:
A total of 227 outpatients were prospectively randomized and treated with a neutral wedged insole inserted into shoes (placebo with shoes; n=45), a wedged insole inserted into shoes (inserted insole with shoes; n=45), a sock-type ankle supporter with a wedged insole when wearing socks or flat footwear (inserted insole without shoes; n=46), a subtalar strapped insole when wearing shoes (strapped insole with shoes; n=45), and the strapped insole with socks or flat footwear (strapped insole without shoes; n=46). The Lequesne index of knee OA at week 12 was compared with the baseline in each treatment group.
RESULTS:
Twenty patients withdrew from the study, and the 207 patients who completed the 12-week study were evaluated. At the final assessment, participants wearing the inserted insole without shoes (P=0.003), the strapped insole with shoes (P<0.0001), and the strapped insolewithout shoes (P<0.0001) demonstrated significantly improved Lequesne index scores in comparison with their baseline assessments. No significant differences were found in the placebo (P=0.16) or the inserted insole with shoes (P=0.2) groups.
CONCLUSION:
Concomitant heeled footwear may decrease the efficacy of an inserted lateral wedged insole. The optimal usage of a lateral wedgedinsole for knee OA would be the combination with socks or flat footwear without heels.
Arthritis Rheum. 2007 Apr;56(4):1198-203.
A randomized crossover trial of a wedged insole for treatment of knee osteoarthritis.
Baker K, Goggins J, Xie H, Szumowski K, LaValley M, Hunter DJ, Felson DT.
Source
Veterans Affairs Boston Health Care System, Boston University Medical School, Massachusetts 02118, USA. krbaker@bu.edu
Abstract
OBJECTIVE:
In uncontrolled studies, a lateral-wedge insole has reduced knee pain in patients with medial knee osteoarthritis (OA). The aim of this study was to test the efficacy of this simple, low-cost intervention for pain in patients with medial knee OA.
METHODS:
We conducted a double-blind, randomized, crossover trial designed to detect a small effect of treatment. Participants were at least 50 years of age and had medial joint space narrowing on posteroanterior semiflexed radiographs and scores indicating moderate pain for 2 of the 5 items on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain scale. Participants were randomized to receive a 5 degrees lateral-wedge insole or a neutral insole for 6 weeks. Following a 4-week washout period, participants crossed over to the other treatment for 6 weeks.Knee pain, the primary outcome, was assessed by the WOMAC pain scale (visual analog scale version). Secondary outcomes included the WOMAC disability subscale, overall knee pain, 50-feet walk time, chair-stand time, and use of medications for knee pain.
RESULTS:
Ninety patients were randomized. The mean difference in pain between the 2 treatments was 13.8 points on the WOMAC pain scale (95% confidence interval -3.9, 31.4 [P=0.13]). We observed similar small effects for the secondary outcomes.
CONCLUSION:
The effect of treatment with a lateral-wedge insole for knee OA was neither statistically significant nor clinically important.
Osteoarthritis Cartilage. 2007 Aug;15(8):932-6. Epub 2007 Mar 27.
The lateral wedged insole with subtalar strapping significantly reduces dynamic knee load in the medialcompartment gait analysis on patients with medial knee osteoarthritis.
Kuroyanagi Y, Nagura T, Matsumoto H, Otani T, Suda Y, Nakamura T, Toyama Y.
Source
Department of Orthopaedic Surgery, School of Medicine, Keio University, Tokyo, Japan. yuji-kuro@nifty.com
Abstract
OBJECTIVE:
Two lateral wedged insoles were compared: one with, and the other without, subtalar strapping.
METHODS:
Twenty-one patients (age 58-83, mean 72) with medial knee osteoarthritis (OA) were enrolled. Thirty-seven knees in the patients were divided into three groups based on the Kellgren and Lawrence OA grading system; grades 2 (cases=20), 3 (cases=11), and 4 (cases=6). The subjects were tested during walking barefoot and during walking with a silicon rubber lateral wedged insole with elevation of 10 mm attached to a barefoot. Gait analysis was performed on a 10 m walkway for each subject under three different walking conditions; barefoot, wearing a conventionalinsole, and a subtalar strapping insole. Peak knee varus moment during gait was measured under each condition, and compared between the three conditions and between the OA grades.
RESULTS:
On the whole (cases=37), the peak varus moment was significantly reduced by wearing either of the insoles, compared to walking barefoot. The reduction was more obvious with the strapping insole (-13%, P<0.01), compared with the conventional insole (-8%, P<0.05). In moderate OA patients (grades 2 and 3), the moments were significantly lower with the strapping insole, compared with the conventional insole (P=0.0048 and 0.005, respectively). However, no significant difference was detected in severe OA patients (grade 4) between the two types of insoles (P=0.4).
CONCLUSIONS:
Both lateral wedged insoles significantly reduced the peak medial compartment load during gait. The subtalar strapping insole had a greater effect than the conventional insole, particularly in patients with moderate medial knee OA.
Arch Phys Med Rehabil. 2006 Nov;87(11):1436-41.
Effects of disease severity on response to lateral wedged shoe insole for medial compartment knee osteoarthritis.
Shimada S, Kobayashi S, Wada M, Uchida K, Sasaki S, Kawahara H, Yayama T, Kitade I, Kamei K, Kubota M, Baba H.
Source
Gait Analysis Laboratory, Division of Physical Therapy and Rehabilitation, Fukui University Hospital, Fukui, Japan. sshima@fmsrsa.fukui-med.ac.jp
Abstract
OBJECTIVE:
To determine the effects of lateral wedged insoles on knee kinetics and kinematics during walking, according to radiographic severity ofmedial compartment knee osteoarthritis (OA).
DESIGN:
A prospective case control study of patients with medial compartment OA of the knee.
SETTING:
Gait analysis laboratory in a university hospital.
PARTICIPANTS:
Forty-six medial compartment knees with OA of 23 patients with bilateral disease and 38 knees of 19 age-matched healthy subjects as controls.
INTERVENTIONS:
Not applicable.
MAIN OUTCOME MEASURES:
We measured the peak external adduction moment at the knee during the stance phase of gait and the first acceleration peak after heel strike at the lateral side of the femoral condyles. Kellgren and Lawrence grading system was used for radiographic assessment of OA severity.
RESULTS:
The mean value of peak external adduction moment of the knee was higher in OA knees than the control. Application of lateral wedgedinsoles significantly reduced the peak external adduction moment in Kellgren-Lawrence grades I and II knee OA patients. The first acceleration peak value after heel strike in these patients was relatively high compared with the control. Application of lateral wedged insoles significantly reduced the first acceleration peak in Kellgren-Lawrence grades I and II knee OA patients.
CONCLUSIONS:
The kinetic and kinematic effects of wearing of lateral wedged insoles were significant in Kellgren-Lawrence grades I and II knee OA. The results support the recommendation of use of lateral wedged insoles for patients with early and mild knee OA.
Osteoarthritis Cartilage. 2006 Mar;14(3):231-7. Epub 2005 Nov 3.
A 2-year follow-up of a study to compare the efficacy of lateral wedged insoles with subtalar strapping and in-shoe lateral wedged insoles in patients with varus deformity osteoarthritis of the knee.
Source
Toda Orthopedic Rheumatology Clinic, Suita, Osaka, Japan. ugj72766@nifty.com
Abstract
OBJECTIVE:
This study was conducted in order to assess the effect of wearing a lateral wedged insole with a subtalar strap for 2 years in patients with osteoarthritis varus deformity of the knee (knee OA).
DESIGN:
The setting was an outpatient clinic. The efficacies of the strapped insole and a traditional shoe insert wedged insole (the inserted insole), as a positive control, were compared at the baseline and after 2 years of treatment. Randomization was performed according to birth date. The 61 female outpatients with knee OA who completed a prior 6-month study were asked to wear their respective insoles continuously as treatment during the course of the 2-year study. The femorotibial angle (FTA) was assessed by standing radiographs obtained while the subjects were barefoot and the Lequesne index of the knee OA at 2 years was compared with those at baseline in each insole group.
RESULTS:
There were 61 patients in the original study, but 13 patients (21.3%) did not want to wear the insole continuously and five (8.2%) withdrew for other reasons. The 42 patients who completed the 2-year study were evaluated. At the 2-year assessment, participants wearing the subtalar strapped insole (n=21) demonstrated significantly decreased FTA (P=0.015), and significantly improved Lequesne index (P=0.031) in comparison with their baseline assessments. These significant differences were not found in the group with the traditional shoe inserted wedged insole (n=21).
CONCLUSION:
Only those participants using the subtalar strapped insole demonstrated significant change in the FTA in comparison with the baseline assessments. If the insole with a subtalar strap maintains FTA for more than 2 years, it may restrict the progression of degenerative articular cartilage lesions of knee OA.
Arthritis Rheum. 2004 Oct;50(10):3129-36.
A six-month followup of a randomized trial comparing the efficacy of a lateral-wedge insole with subtalarstrapping and an in-shoe lateral-wedge insole in patients with varus deformity osteoarthritis of the knee.
Source
Toda Orthopedic Rheumatology Clinic, Suita, Osaka, Japan. fwjh2766@mb.infoweb.ne.jp
Abstract
OBJECTIVE:
To assess the effect of a lateral-wedge insole with elastic strapping of the subtalar joint on the femorotibial angle in patients with varusdeformity of the knee.
METHODS:
The efficacy of a wedged insole with subtalar straps and that of a traditional wedged insole shoe insert were compared. Sixty-six female outpatients with knee osteoarthritis (OA) were randomized (according to birth date) to be treated with either the strapped or the traditional insertedinsole. Standing radiographs with unilateral insole use were used to analyze the femorotibial angles for each patient. In both groups, the baseline and 6-month visual analog scale (VAS) scores for subjective knee pain and the Lequesne index scores for knee OA were compared.
RESULTS:
The 61 patients who completed the 6-month study were evaluated. At baseline, there was no significant difference in the femorotibial angle (P = 0.66) and the VAS score (P = 0.75) between the 2 groups. At the 6-month assessment, the 29 subjects wearing the subtalar-strapped insoledemonstrated a significantly decreased femorotibial angle (P < 0.0001) and significantly improved VAS scores (P = 0.001) and Lequesne index scores (P = 0.033) compared with their baseline assessments. These significant differences were not observed in the 32 subjects assigned to the traditional shoe-inserted wedged insole.
CONCLUSION:
These results suggest that an insole with a subtalar strap maintained the valgus correction of the femorotibial angle in patients withvarus knee OA for 6 months, indicating longer-term clinical improvement with the strapped insert compared with the traditional insert.
Arch Phys Med Rehabil. 2004 Apr;85(4):673-7.
The effects of different elevations of laterally wedged insoles with subtalar strapping on medial compartmentosteoarthritis of the knee.
Source
Toda Orthopedic Rheumatology Clinic, Suita, Osaka, Japan.
Abstract
OBJECTIVE:
To assess the radiographic and symptomatic effects of treating patients with medial compartment osteoarthritis (OA) of the knee with laterally wedged insoles with subtalar strapping of varying elevations.
DESIGN:
Prospective quasi-experimental evaluation.
SETTING:
Outpatient clinic in Japan.
PARTICIPANTS:
Sixty-two women outpatients with knee OA who were randomized into 3 groups according to their birth dates and wedge elevation.
INTERVENTIONS:
Participants wore laterally wedged insoles with subtalar strapping with elevations of 8, 12, or 16 mm for 2 weeks.
MAIN OUTCOME MEASURES:
Standing radiographs were used to analyze the femorotibial angle for each subject, both with and without their respective unilateral insoles. The remission scores of the Lequesne index of severity for knee OA were compared among the 3 groups at the conclusion. Participants were asked to report adverse effects on use of the insoles.
RESULTS:
The 16-mm group (n=21) showed a significantly greater valgus correction of the femorotibial angle than the 8-mm group (n=20) (P=.013). The remission score was significantly improved in the 12-mm group (n=21) compared with the 16-mm group (P=.029). Adverse effects were more common in the 16-mm group (9/21, 42.8%) than in the 12-mm (3/21, 14.3%) or 8-mm (2/20, 10%) groups.
CONCLUSIONS:
The degree of change in femorotibial angle with the insole with subtalar strapping was affected by the tilt of the lateral wedge. For constant routine use, the 8- or 12-mm elevation wedged insoles with subtalar strapping may be more comfortable and effective than the 16-mm elevation wedge.
Osteoarthritis Cartilage. 2004 Jan;12(1):46-55.
Laterally elevated wedged insoles in the treatment of medial knee osteoarthritis. A two-year prospectiverandomized controlled study.
Pham T, Maillefert JF, Hudry C, Kieffert P, Bourgeois P, Lechevalier D, Dougados M.
Source
René Descartes University, Cochin Hospital, Paris, France.
Abstract
OBJECTIVE:
To compare the clinical effects of laterally wedged insoles and neutrally wedged insoles (used as control) in patients with medialfemoro-tibial knee osteoarthritis.
METHODS:
Study design: 24-month prospective randomized controlled study. Patients: Outpatients with painful medial femoro-tibial knee osteoarthritis. Outcome measures: Patient’s overall assessment of disease activity (5 grade scale), WOMAC index subscales and concomitant treatments. Statistical analysis: Performed as an intention-to-treat analysis, with the last observation carried forward (LOCF). Main symptomatic criterion: Improvement in the patient’s assessment of activity (defined as a reduction of one grade or more at the end of the study as compared to baseline, and no intra-articular injection or lavage during the 6 months previous to the last visit). Secondary criteria for assessment: (a) Changes in the WOMAC subscales at month 24, and (b) concomitant therapies (analgesics, NSAIDs and intra-articular injections or lavages). Structural criterion: Joint space width (JSW) at the narrowest point. Non-compliance was defined as intermittent or lack of insole fitting at two consecutive visits. Compliance within groups was compared by using a life table analysis technique (Log-Rank).
RESULTS:
The baseline characteristics of the 156 recruited patients (41 males, 115 females, mean age 64.8 years) were not different in the 2treatment groups. At year 2, there was no statistically significant difference between the 2 groups concerning the percentages of patients with improvement in both global assessment of disease activity and in WOMAC subscales (pain, stiffness, function). The number of days with NSAIDs intake was lower in the group with laterally wedged insoles than in the neutrally wedged group (71+/-173 days vs. 127+/-193 days, P=0.003, Mann-Whitney test). The mean joint space narrowing rate did not differ between the two groups: 0.21+/-0.59 mm/year in the laterally wedged group vs 0.12+/-0.32 mm/year in the neutrally wedged group. Compliance and tolerance were satisfactory. Compliance was different between the 2 groups at month 24, with a greater frequency of patients who wore insoles permanently in the laterally wedged insole group than in the other group (85.8% vs 71.9%, P=0.023).
CONCLUSION:
This study failed to demonstrate a relevant symptomatic and/or structural effect of laterally-wedged insoles in medial femoro-tibial OA. However, the reduced NSAIDs intake and the better compliance in the treatment group are in favor of a beneficial effect of laterally-wedged insoles inmedial femoro-tibial OA.
Arthritis Rheum. 2002 Oct 15;47(5):468-73.
Usefulness of an insole with subtalar strapping for analgesia in patients with medial compartment osteoarthritis of the knee.
Source
Toda Orthopedic Rheumatology Clinic, Suita, Osaka, Japan. fwjh2766@mb.infoweb.ne.jp
Abstract
OBJECTIVE:
To assess the effect of an insole with subtalar strapping on patients with medial compartment osteoarthritis (OA) of the knee.
METHODS:
Novel lateral wedged insoles with elastic subtalar strapping (the subtalar strapping support group) and ankle supporters with a lateral wedged heel insert (the sock-type ankle support group) were prepared. Eighty-eight female outpatients with knee OA were treated with 1 of the 2 insoles for 8 weeks. Femorotibial angle was assessed by standing radiographs with and without unilateral insole use for each subject. Symptoms ofknee OA were evaluated according to the severity index of Lequesne et al at baseline and at the final assessment.
RESULTS:
Participants wearing the insole with subtalar strapping (n = 42) demonstrated significantly decreased femorotibial angle (an average of change: -3.1 degrees +/- 2.5 degrees, P < 0.0001), but a significant difference was not found in the sock-type ankle support group (n = 46; -0.4 degrees +/- 1.1 degrees, P > 0.05). In the subtalar strapping support group, pain during bed rest with full extension of the knee (P < 0.0001), pain after getting up (P = 0.04), pain on getting up from a seated position (P = 0.021), maximum distance walked (P = 0.009), and aggregate severity score (P < 0.0001) were significantly improved compared with baseline. In contrast, significant symptomatic improvement was detected only in the aggregate score (P = 0.016) in the sock-type ankle support group, but not in any of the 10 specific categories.
CONCLUSION:
The lateral wedged insole with subtalar strapping induces correction of the femorotibial angle and symptomatic relief in patients with varus-deformity knee OA.
J Rheumatol. 2001 Dec;28(12):2705-10.
Effect of a novel insole on the subtalar joint of patients with medial compartment osteoarthritis of the knee.
Toda Y, Segal N, Kato A, Yamamoto S, Irie M.
Source
Toda Orthopedic Rheumatology Clinic, Suita, Osaka, Japan. fwjh2766@mb.infoweb.ne.jp
Abstract
OBJECTIVE:
To assess the efficacy of a lateral wedge insole with elastic strapping of the subtalar joint for conservative treatment of osteoarthritis(OA) of the knee.
METHODS:
The efficacy of a novel insole with elastic subtalar strapping and a traditional shoe insert wedge insole was compared. Ninety female outpatients with OA of the knee were treated with wedge insoles for 8 weeks. Randomization was performed according to birth date. Standing radiographs with unilateral insole use were used to analyze the femorotibial and talar tilt angles for each patient with and without their respectiveinsole. Visual analog scale (VAS) score for subjective knee pain at the final assessment was compared with that at baseline in both groups.
RESULTS:
Participants wearing the elastically strapped insole (n = 46) had significantly decreased femorotibial angle (p < 0.0001) and talar tilt angle (p = 0.005) and significantly improved VAS pain score (p = 0.045) in comparison with baseline assessments. These significant differences were not found in the group with the inserted insole (n = 44).
CONCLUSION:
The novel strapped insole leads to valgus angulation of the talus, resulting in correction of the femorotibial angle in patients with kneeOA with varus deformity, and may have a therapeutic effect similar to that of high tibial osteotomy.
Resumos relacionados à fratura por estresse:
Injury. 1990 Sep;21(5):275-9.
Fatigue fractures of the foot
Department of Orthopaedic Surgery, Western Infirmary, Glasgow, UK
http://dx.doi.org/10.1016/0020-1383(90)90039-W, How to Cite or Link Using DOI
Abstract
While fatigue fractures are common in military practice they are much less so in civilian practice and thus tend to be overlooked. Fractures occur most commonly in the distal second and third metatarsal shafts and within the calcaneum, but occur in almost any other bone of the foot. Any suspicious history of repetitive stress or sudden change in activity, athletic or otherwise, associated with swelling and point tenderness warrants further investigation by bone scintigraphy. Attention is drawn to the importance of understanding the basic biomechanical function of the foot and how it may affect the development of fatigue fractures. A distinction is drawn between the distal fractures of the second and third metatarsal shafts and those occurring in the proximal shafts of any of the metatarsals which have a different aetiology. Following conventional management in a plaster cast, it is suggested that any biomechanical anomaly which is present is compensated appropriately with an orthotic insole.
Scand J Med Sci Sports. 2011 Dec;21(6):804-8. doi: 10.1111/j.1600-0838.2010.01116.x. Epub 2010 May 12.
Can orthotic insoles prevent lower limb overuse injuries? A randomized-controlled trial of 228 subjects.
Mattila VM, Sillanpää PJ, Salo T, Laine HJ, Mäenpää H, Pihlajamäki H.
Source
Centre of Military Medicine, Lahti, Finland. ville.mattila@uta.fi
Abstract
Lower limb overuse injuries are common among people who are exposed to physical stress. Orthotic shoe insoles are widely used to prevent lower limb overuse injuries. Here, we conducted a randomized-controlled study to examine whether the use of orthotic insoles prevents lower limb overuse injuries. Participants (n=228) were randomly assigned to use (n=73) or not to use (n=147) orthotic insoles. The insoles were molded to the shape of the foot to provide support during physical activity. The main outcome measure in the present study was the physician-diagnosed lower limb overuse injury. Thirty-four (46.6%) subjects in the insole group were diagnosed with a lower limb overuse injury compared with 56 (38.1%) in the control group (P=0.29) during the 6-month study period. When body mass index and the results of a 12-min running test and muscle strength were adjusted in a Cox’s regression model, the hazard ratio for lower limb overuse injury in the insole group was 1.3 (95% confidence intervals: 0.8-2.1) compared with the control group. Use of orthotic insoles was not associated with a decrease in lower limb overuse injuries. Our findings suggest that routine use of orthotic insoles does not prevent physical-stress-related lower limb injuries in healthy young male adults.
Am J Public Health. 1988 Dec;78(12):1563-7.
Prevention of lower extremity stress fractures: a controlled trial of a shock absorbent insole.
Gardner LI Jr, Dziados JE, Jones BH, Brundage JF, Harris JM, Sullivan R, Gill P.
Source
Department of Epidemiology, Walter Reed Army Institute of Research, Washington, DC 20307-5100.
Abstract
A prospective controlled trial was carried out to determine the usefulness of a viscoelastic polymer insole in prevention of stress fractures and stressreactions of the lower extremities. The subjects were 3,025 US Marine recruits who were followed for 12 weeks of training at Parris Island, South Carolina. Polymer and standard mesh insoles were systematically distributed in boots that were issued to members of odd and even numbered platoons. The most important finding was that an elastic polymer insole with good shock absorbency properties did not prevent stress reactions of bone during a 12-week period of vigorous physical training. To control for the confounding effects of running in running shoes, which occurred for about one and one-half hours per week for the first five weeks, we also examined the association of age of shoes and cost of shoes with injury incidence. A slight trend of increasing stress injuries by increasing age of shoes was observed. However, this trend did not account for the similarity of rates in the two insole groups. In addition, we observed a strong trend of decreasing stress injury rate by history of increasing physical activity, as well as a higherstress injury rate in White compared to Black recruits. The results of the trial were not altered after controlling for these factors. This prospective study confirms previous clinical reports of the association of stress fractures with physical activity history. The clinical application of a shockabsorbing insole as a preventive for lower extremity stress reactions is not supported in these uniformly trained recruits. The findings are relevant to civilian populations.
Resumos sobre análise de pressão plantar:
Prosthet Orthot Int. 2008 Sep;32(3):356-62. doi: 10.1080/03093640802016159.
Comparison of plantar pressure distribution patterns between foot orthoses provided by the CAD-CAM and foam impression methods.
Source
Department of Health Technology and Informatics, The Hong Kong Polytechnic University, Hong Kong, China.
Abstract
Foot orthotic treatment is one of the major conservative methods used to handle foot problems. Total plantar contact foot orthoses are used to reduce and redistribute peak pressures. For the fabrication of a total plantar contact foot orthosis, the computer-aided design and computer-aided manufacturing (CAD-CAM) method has been applied. In this study, the plantar foot-orthosis interface pressure data during walking were collected by the Novel Pedar-mobile in-shoe plantar pressure measuring system. The data were collected under three conditions: (i) Flat insole, (ii) foot orthosis provided by the CAD-CAM method, and (iii) foot orthosis provided by the foam impression method. The Swiss Comfort CAD-CAM foot orthotics system was used in this study. For conditions (ii) and (iii), foot shapes were collected in partial weight bearing and subtalar neutral conditions. Thirty normal subjects were recruited for this study. The plantar foot surface was divided into eight plantar foot regions and then was investigated. These regions included the heel, the medial and lateral arches, the medial, mid and lateral forefoot, the hallux, and the lateral toes. The results showed that the orthoses provided by both the CAD-CAM and foam impression methods could decrease the peak pressure and the maximum force in the heel region, and increase the peak pressure and the maximum force in the medial arch region. Both orthoses redistributed the peak pressure and the maximum force from the heel to the medial arch region. The peak pressure in the mid forefoot region was different between the orthoses provided by the CAD-CAM and foam impression methods.
J R Soc Med. 2006 Jan;99(1):32-7.
Do shock absorbing insoles in recruits undertaking high levels of physical activity reduce lower limb injury? A randomized controlled trial.
Withnall R, Eastaugh J, Freemantle N.
Source
Regional Medical Centre & Regional Rehabilitation Unit, RAF Halton, Aylesbury, Bucks HP22 5PG, UK. richwithnall@doctors.org.uk
Abstract
OBJECTIVES:
To assess the benefits, if any, of the use of shock absorbing insoles in reducing lower limb injury among Air Force recruits, and to assess the differences, if any, in the efficacy of two commonly available shock absorbing insoles.
DESIGN:
Randomized controlled trial.
SETTING:
RAF Halton, UK. Site of all basic training for RAF personnel.
PARTICIPANTS:
1205 recruits participating in basic training between 17 September 2003 and 7 April 2004.
INTERVENTIONS:
Participants were randomized to receive either standard issue Saran non-shock absorbing insoles, or shock absorbing Sorbothane or Poron insoles, on a 1:1:1 basis.
MAIN OUTCOME MEASURES:
The primary outcome measure was withdrawal from training for lower limb injury. The two primary comparisons were shock absorbing insole versus non-shock absorbing insole, and Sorbothane versus Poron (comparison of different shock absorbing insoles). Secondary outcomes were medical withdrawals for reasons other than those qualifying for the primary outcome measure.
RESULTS:
When comparing the non-shock absorbing insole to the shock absorbing insoles 72/401 participants (18.0%) allocated to Saran insoles were removed from training because of a qualifying lower limb injury, compared with 149/804 (18.5%) allocated to the shock absorbing insole (Sorbothane or Poron), odds ratio 1.04 (95% CI 0.75 to 1.44; P=0.87). When comparing the two shock absorbing insole 73/421 participants (17.3%) randomized to Sorbothane were removed from training because of a qualifying lower limb injury, compared with 76/383 for Poron (19.8%), odds ratio 0.85 (95% CI 0.58 to 1.23; P=0.37).
CONCLUSIONS:
Similar rates of lower limb injuries were observed for all insoles (shock absorbing and non-shock absorbing) in the trial. The trial provides no support for a change in policy to the use of shock absorbing insoles for military recruits.
Mil Med. 2004 Sep;169(9):741-6.
User trial and insulation tests to determine whether shock-absorbing insoles are suitable for use by militaryrecruits during training.
House CM, Dixon SJ, Allsopp AJ.
Source
Institute of Naval Medicine, Alverstoke, Hants PO12 2LJ, U.K.
Abstract
A user trial was undertaken to determine whether a shock-absorbing insole is suitable for military use. Two thicknesses of insole (3 mm and 6 mm) were studied and were issued to 38 Royal Marine recruits to wear in their military boots for weeks 12 to 30 of training. Biomechanical measurements showed that both thicknesses of insole significantly (p < 0.05) attenuated the peak pressures generated at heel strike and during forefoot loading when new (relative to a no-insole condition) and that this was well maintained after wear. This was supported by mechanical tests conducted on theinsoles. It was concluded that the insoles are sufficiently durable for military use. The main user complaint was that water retention reduced the comfort of the insoles; however, insulation tests conducted with a foot manikin indicated that switching from the current-issue Saran insoles to thetrial insoles would not increase the risk of recruits sustaining nonfreezing cold injuries to their feet.
Gait Posture. 2002 Dec;16(3):297-303.
The influence of simulated wear upon the ability of insoles to reduce peak pressures during running when wearing military boots.
House CM, Waterworth C, Allsopp AJ, Dixon SJ.
Source
Institute Naval Medicine, Alverstoke, Gosport, UK. hsosurv@inm.mod.uk
Abstract
Mechanical degradation of three types of shock absorbing insoles equivalent to 100-130 km of running did not reduce their ability to attenuate the peak pressures generated during running when wearing military boots. Pressure measurements at the heel and forefoot were recorded with pressure measuring insoles placed in the boots of nine subjects. Two of the three insoles tested reduced the peak pressures (P<0.05) generated at the heel and forefoot relative to the no-insole (control) condition. The most effective insole reduced the peak pressures at the heel by 37% and at the forefoot by 24%.
J Am Podiatr Med Assoc. 2000 Oct;90(9):441-9.
Effect of cast and noncast foot orthoses on plantar pressure and force during normal gait.
Redmond A, Lumb PS, Landorf K.
Source
Division of Podiatry, University of Western Sydney, Campbelltown, New South Wales, Australia.
Abstract
A variety of plantar pressure and force measures were explored in 22 healthy individuals with excessive pronation. The measures were obtained while the subjects wore a thin-soled athletic shoe alone, a modified Root foot orthosis made from a neutral cast, and a flat noncast insole with a 6 degrees varus rearfoot post. The data obtained from subjects wearing the noncast insole differed only minimally from those obtained while they were wearing the shoe only. In contrast, the modified Root orthosis had a profound effect on foot function. Heel forces and pressures were reduced, and the rearfoot contact area was increased. Measures of force in the midfoot demonstrated substantial increases in load in this region, but the increase in area associated with the contoured device resulted in no increase in midfoot pressure measurements. Forefoot pressures were reduced both medially and laterally with the cast device in place.
Gait Posture. 1999 Mar;9(1):31-7.
The shock attenuation characteristics of four different insoles when worn in a military boot during running and marching.
Windle CM, Gregory SM, Dixon SJ.
Source
Institute Naval Medicine, Alverstoke, Gosport PO12 2DL, UK. yj72@dial.pipex.com
Abstract
A study was undertaken to determine if placing shock absorbing insoles in the boots of Royal Marine recruits would attenuate the peak pressure at the foot-boot interface, when marching at 4.8 kph carrying a 32 kg (70 lb) Bergen and running at 12.8 kph in loose order plus webbing weighing 10 kg (22 lb). Four types of insoles were assessed: viscoelastic polymetric insole (Cambion(R)) polymetric foam insole (PPT(R)) Saran insole (militaryissue) and Sorbothane(R). There was a fifth control condition in which no insoles were used. Pressure measurements during heel strike and forefoot loading were taken using Paratec equipment with pressure measuring insoles placed in the boots. Data were obtained from eleven subjects and indicated that all the insoles significantly (P<0.05) attenuated the peak pressures generated during heel strike and forefoot loading. The performance of the four insoles in terms of peak pressure attenuation ranked in order with the best first were: Sorbothane Cambion PPT Saran. The Sorbothane insole was substantially and significantly (P<0.05) better than the other insoles in terms of attenuating peak pressures during heel strike. Duringrunning, mean peak pressure at heel strike was 494 kPa in the control condition, this was reduced to 377 kPa when wearing Sorbothane insoles (a reduction of 27%). When marching the Sorbothane insoles reduced the mean peak pressure at heel strike from 395 kPa (control) to 303 kPa (23% reduction). During forefoot loading the peak pressure attenuation of all four insoles was similar, although on average the Sorbothane insole performed slightly better than the others and was significantly different (P<0. 05) to the Cambion insole. Mean peak forefoot loading pressure in the control condition when running was 413 kPa, with the Sorbothane insole it was 367 kPa, during marching the respective mean peak pressures were 397 and 323 kPa. It is concluded that of the four types of insoles assessed the Sorbothane insoles attenuated the greatest amounts of the peak pressure generated at heel strike and during forefoot loading when running and marching wearing military boots.
Arch Phys Med Rehabil. 1999 Jul;80(7):801-4.
Use of computerized insole sensor system to evaluate the efficacy of a modified ankle-foot orthosis forredistributing heel pressures.
Randolph AL, Nelson M, deAraujo MP, Perez-Millan R, Wynn TT.
Source
Department of Physical Medicine and Rehabilitation, New York Medical College, Valhalla 10595, USA.
Abstract
OBJECTIVE:
Evaluation of orthosis purported to decrease pressure on the heel while walking.
DESIGN:
The Multipodus System is an orthotic device, designed for this purpose, that can be worn with flat or rocker bottom boot. Ten subjects underwent four trials: first, an initial walk wearing their usual shoes, then using the orthosis on the left, with a flat bottom boot, then with a rocker bottom boot, and a final walk. Pressures exerted on the plantar surface of the hindfoot, midfoot, and forefoot were measured electronically and analyzed.
SETTING AND PARTICIPANTS:
Ten consecutive normal subjects were tested on a conventional tile floor in a gait laboratory.
RESULTS:
Peak pressures in the initial walk averaged: heel, 9.6 +/- 2.3psi; midfoot, 2.6 +/- 1.7psi; and forefoot, 10.3 +/- 2.6psi. Pressures on the foot were redistributed significantly when the orthosis was used. Heel pressure was reduced significantly compared to the ordinary shoes using both the flat bottom boot (5.0 +/- 1.2psi, a decrease of 48% [p = .0001]) and the rocker bottom boot (4.5 +/- 1.5psi, a decrease of 53% [p = .0001]). Pressure was increased at the midfoot with both the flat bottom boot (6.6 +/- 3.2psi, an increase of 61% [p = .0001]) and the rocker bottom boot (6.8 +/- 2.9psi, an increase of 62% [p = .0001]). Pressures at the forefoot decreased 19% (8.3psi) with the flat bottom boot and 32% (7.0psi; p = .0003) with the rocker bottom boot.
CONCLUSIONS:
Redistribution of pressure on the foot with orthosis is characterized by reduction at the hindfoot and forefoot and increase at the midfoot with both the flat and rocker bottom boots, thereby promoting healing of calcaneal and forefoot ulcers. The integrity of the midfoot, however, must not be compromised.
Resumos relacionados à prática de esportes:
Clin Rehabil. 2011 Oct;25(10):913-23. doi: 10.1177/0269215511411938. Epub 2011 Jul 25.
Application of wedged foot orthosis effectively reduces pain in runners with pronated foot: a randomized clinical study.
Source
Department of Physical Therapy and Assistive Technology, National Yang-Ming University, Taipei, Taiwan.
Abstract
OBJECTIVE:
To examine the effects of foot orthosis intervention during a 60-minute running test in pronated-foot runners with overuse knee or foot pain during running.
DESIGN:
A randomized, controlled design.
SETTING:
Sports gym.
PARTICIPANTS:
Twenty-four runners with pronated foot who experienced pain over anterior knee or foot region during running were recruited and randomized into the treatment, or the control, group.
INTERVENTIONS:
A soft insole with a semi-rigid rearfoot medial wedge was given to the treatment group, and a soft insole without corrective posting was applied to the control group.
OUTCOME MEASURES:
The immediate and short-term effects of orthosis application on incidence of pain, pain intensity and onset time were evaluated using the 60-minutes treadmill test.
RESULTS:
Immediately after wearing the foot orthosis, pain incidence reduced in the treatment group but not in the control group (P = 0.04). After two weeks, seven (58%) subjects in the treatment group and one (8%) in the control group were free of pain during the test (P = 0.01). The pain intensity score decreased significantly after orthosis application, from 35.5 to 17.2 (immediate effect, P = 0.014), then to 12.3 (short-term effect, P < 0.001).
CONCLUSION:
The rearfoot medially-wedged insole was a useful intervention for preventing or reducing painful knee or foot symptoms during running in runners with pronated foot.
J Am Podiatr Med Assoc. 2008 Jan-Feb;98(1):36-41.
Effect of cushioned insoles on impact forces during running.
O’Leary K, Vorpahl KA, Heiderscheit B.
Source
Sports Rehabilitation Clinic, University of Wisconsin Hospital and Clinics, Madison, USA.
Abstract
BACKGROUND:
The use of cushioned or shock-absorbing insoles has been suggested as a mechanism to reduce the impact forces associated with running, thereby protecting against overuse injuries. The purpose of this study was to determine whether the use of cushioned insoles reduced impact forces during running in healthy subjects.
METHODS:
Sixteen recreational runners (9 females and 7 males) ran at a self-selected pace for five trials with and without the use of cushioned insoles. During each trial, ground reaction forces, tibial accelerations, lower-extremity kinematics, and subject-perceived comfort were recorded. All variables were tested with the level of statistical significance set at alpha = .05.
RESULTS:
The use of cushioned insoles resulted in significant reductions in mean vertical ground reaction force peak impact (6.8%) and ground reaction force loading rate (8.3%), as well as peak tibial acceleration (15.8%). Spectral analysis of the tibial acceleration data in the frequency range associated with impact accelerations (12-25 Hz) revealed no change in the predominant frequency or the power of the predominant frequency. The knee flexion angle at initial contact and perceived comfort were similar for the two conditions.
CONCLUSIONS:
This study demonstrates the effectiveness of one type of cushioned insole in reducing peak impact force and tibial acceleration at initial foot-ground contact during running. The impact reduction observed was independent of knee kinematic adjustments or changes in perceived comfort. Further study is required to determine whether the reduction in loading that accompanied the use of the cushioned insoles can affect the incidence of running-related injuries.
Resumos relacionados à equilíbrio e instabilidade:
J Safety Res. 2011 Dec;42(6):473-85. doi: 10.1016/j.jsr.2011.02.002. Epub 2011 Nov 10.
Reducing fall risk by improving balance control: development, evaluation and knowledge-translation of new approaches.
Maki BE, Sibley KM, Jaglal SB, Bayley M, Brooks D, Fernie GR, Flint AJ, Gage W, Liu BA, McIlroy WE, Mihailidis A, Perry SD, Popovic MR, Pratt J, Zettel JL.
Source
Sunnybrook Health Sciences Centre, Toronto, Canada. brian.maki@sri.utoronto.ca
Abstract
PROBLEM:
Falling is a leading cause of serious injury, loss of independence, and nursing-home admission in older adults. Impaired balance control is a major contributing factor.
METHODS:
Results from our balance-control studies have been applied in the development of new and improved interventions and assessment tools. Initiatives to facilitate knowledge-translation of this work include setting up a new network of balance clinics, a research-user network and a research-user advisory board.
RESULTS:
Our findings support the efficacy of the developed balance-training methods, balance-enhancing footwear, neuro-prosthesis, walker design, handrail-cueing system, and handrail-design recommendations in improving specific aspects of balance control. IMPACT ON KNOWLEDGE USERS: A new balance-assessment tool has been implemented in the first new balance clinic, a new balance-enhancing insole is available through pharmacies and other commercial outlets, and handrail design recommendations have been incorporated into 10 Canadian and American building codes. Work in progress is expected to have further impact.
J Gerontol A Biol Sci Med Sci. 2008 Jun;63(6):595-602.
Efficacy and effectiveness of a balance-enhancing insole.
Perry SD, Radtke A, McIlroy WE, Fernie GR, Maki BE.
Source
Department of Kinesiology and Physical Education, Wilfrid Laurier University, Ontario, Canada. sperry@wlu.ca
Abstract
BACKGROUND:
Age-related loss of foot-sole cutaneous sensation is very common and is associated with impaired balance control. This study investigated the effect of a balance-enhancing insole (designed to facilitate foot-sole sensation) on lateral gait stability and evaluated its effectiveness in daily life.
METHODS:
Forty community-dwelling older adults (age 65-75) with moderate loss of foot-sole sensation (unrelated to neuropathy) were fitted with the same model of walking shoes. Half of the participants were assigned, at random, to wear the shoes with a facilitatory insole for 12 weeks; the other participants wore a conventional insole. A gait perturbation protocol, simulating uneven terrain, was performed at baseline and after wearing the assigned insoles for 12 weeks. Participants were tested with both types of insoles during each gait-testing session and sent in weekly postcards with information pertaining to insole comfort, hours of wear, and falls.
RESULTS:
The facilitatory insole improved lateral stability during gait, and this benefit did not habituate after 12 weeks of wearing the insole in daily life. Nine participants who wore conventional insoles experienced one or more falls, whereas only five of the facilitatory group fell. Although there were initial reports of mild discomfort in 10 cases, all but one participant tolerated the facilitatory insole, and most indicated that they would like to continue wearing the insole on a long-term basis.
CONCLUSIONS:
A relatively simple change in insole design can help to counter effects of age-related (non-neuropathic) decline in foot-sole sensitivity, and is a viable intervention to enhance balance control.
Br J Sports Med 2003;37:170–175
Football boot insoles and sensitivity to extent of ankle inversion movement
G Waddington, R Adams
Background: The capacity of the plantar sole of the foot to convey information about foot position is reduced by conventional smooth boot insoles, compared with barefoot surface contact.
Objective: To test the hypothesis that movement discrimination may be restored by inserting textured replacement insoles, achieved by changing footwear conditions and measuring the accuracy of judgments of the extent of ankle inversion movement.
Methods: An automated testing device, the ankle movement extent discrimination apparatus (AMEDA), developed to assess active ankle function in weight bearing without a balance demand, was used to test the effects of sole inserts in soccer boots. Seventeen elite soccer players, the members of the 2000 Australian Women’s soccer squad (34 ankles), took part in the study. Subjects were randomly allocated to start testing in: bare feet, their own football boots, own football boot and replacement insole, and on the left or right side. Subjects underwent six 50 trial blocks, in which they completed all footwear conditions. The sole inserts were cut to size for each foot from textured rubber “finger profile”sheeting.
Results: Movement discrimination scores were significantly worse when subjects wore their football boots and socks, compared with barefoot data collected at the same time. The substitution of textured insoles for conventional smooth insoles in the football boots was found to restore movement discrimination to barefoot levels.
Conclusions: The lower active movement discrimination scores of athletes when wearing football boots with smooth insoles suggest that the insole is one aspect of football boot and sport shoe design that could be modified to provide the sensory feedback needed for accurate foot positioning.
Resumos relacionados à fascite plantar:
Br J Hosp Med. 1987 Dec;38(6):562-3.
The painful heel.
Source
Medway Hospital, Gillingham.
Abstract
The painful heel syndrome is a common complaint of the middle-aged and elderly. Most patients have no associated disease, except obesity, but young men should be carefully evaluated for ankylosing spondylitis or reactive arthritis. The majority of cases respond to appropriate heel padding, corticosteroid injection or a specially designed insole.
J Am Podiatr Med Assoc. 1997 Jan;87(1):11-6.
Evaluation of magnetic foil and PPT Insoles in the treatment of heel pain.
Caselli MA, Clark N, Lazarus S, Velez Z, Venegas L.
Source
Department of Orthopedic Sciences, New York College of Podiatric Medicine, NY, USA.
Abstract
The effect of a magnetic foil placed in the PPT/Rx Firm Molded Insole on the relief of heel pain was determined using the foot function index. Nineteen patients wore the PPT/Rx Firm Molded Insoles with the magnetic foil for 4 weeks and 15 patients wore the same PPT/Rx Firm Molded Insole with nomagnetic foil for the same time. Approximately 60% of patients in both groups reported improvement. There was also no significant difference in the improvement between the magnetic foil group and the PPT/Rx Firm Molded Insole group in their scores on the post-treatment foot function index. These results suggest that the PPT/Rx Firm Molded Insole alone was effective in treating heel pain after only 4 weeks. The magnetic foil offered no advantage over the plain insole.
Outros Artigos:
J Fam Pract. 2011 Mar;60(3):157-8, 168.
Clinical Inquiry. What is the best way to treat Morton’s neuroma?
Schreiber K, Khodaee M, Poddar S, Tweed EM.
Source
Department of Family Medicine, University of Colorado Denver, USA.
Abstract
No single treatment has been identified in the literature. That said, a protocol of stepped care that showed good results in an uncontrolled trial seems reasonable: patient education and foot-wear or insole changes, followed by corticosteroid injections and, finally, surgery (strength of recommendation [SOR]: C, case series). Injecting sclerosing alcohol depends on the provider’s access to and comfort with ultrasound, but the evidence is insufficient to recommend it routinely (SOR: C, case series).
Cochrane Database Syst Rev. 2011 Jan 19;(1):CD008402. doi: 10.1002/14651858.CD008402.pub2.
Foot orthoses for patellofemoral pain in adults.
Hossain M, Alexander P, Burls A, Jobanputra P.
Source
Department of Orthopaedics, North West Wales NHS Trust, Ysbyty Gwynedd Hospital, Bangor, Wales, UK, LL57 2PW.
Abstract
BACKGROUND:
Foot orthoses, which are specially moulded devices fitted into footwear, are one of the treatment options for patellofemoral or anterior knee pain.
OBJECTIVES:
To assess the effects of foot orthoses for managing patellofemoral pain in adults.
SEARCH STRATEGY:
We searched the Cochrane Bone, Joint and Muscle Trauma Group’s Specialised Register (March 2010), the Cochrane Central Register of Controlled Trials (The Cochrane Library 2010, Issue 1), MEDLINE (1950 to March 2010), EMBASE (1980 to 2010 Week 11), CINAHL (1937 to March 2010), trial registers, reference lists and grey literature. No language restriction was applied.
SELECTION CRITERIA:
We included randomised or quasi-randomised clinical studies that compared foot orthoses with flat insoles or another physical therapy intervention. The primary outcomes were knee pain and knee function.
DATA COLLECTION AND ANALYSIS:
Two authors independently selected eligible trials, assessed methodological quality and performed data extraction. We calculated risk ratios and 95% confidence intervals for dichotomous variables, and mean differences with 95% confidence intervals for continuous variables. We pooled data using the fixed-effect model.
MAIN RESULTS:
Two trials with a total of 210 participants were included. Both trials were at some risk of performance bias. One trial had four intervention groups and the other had three. One trial found that foot orthoses when compared with flat insoles (control group) had better results at six weeks in knee pain (participants with global improvement: risk ratio 1.48, 95% confidence interval 1.11 to 1.99), but not at one year follow-up. Participants in the orthoses group reported significantly more minor adverse effects (e.g. rubbing, blistering) compared with the flat insole group (risk ratio 1.87, 95% confidence intervaI 1.21 to 2.91). Both trials in their comparisons of orthoses plus physiotherapy versus physiotherapy alone found no statistically significant differences between the two intervention groups in knee pain or function. Results for knee pain outcomes did not show significant differences between foot orthoses versus physiotherapy. Although participants in the physiotherapy group had consistently better results for the functional index questionnaire, the clinical relevance of these results is uncertain.
AUTHORS’ CONCLUSIONS:
While not robust, the available evidence does not reveal any clear advantage of foot orthoses over simple insoles or physiotherapy for patellofemoral pain. While foot orthoses may help relieve knee pain over the short term, the benefit may be marginal. Patients treated with orthoses are more likely to complain of mild adverse effects and discomfort.
Clin Orthop Relat Res. 1991 Aug;(269):236-40.
Sesamoid disorders and treatment. An update.
Source
Department of Orthopaedics, Kaiser Permanente Hospital, Panorama City, CA 91402.
Abstract
The anatomy, function, and disorders of the hallucal sesamoids show that the diagnosis and current concept of management are based on the individual patient’s problems. The treatment should always be initiated in a conservative fashion, generally using a molded insole with an appropriate excavation to shift weight from a painful sesamoid. The advantages and disadvantages of sesamoidectomy are influenced by surgical technique. Care in handling the medial and lateral hallucal nerves is essential. Removal of both the medial and lateral sesamoids invariably leads to an intractable clawtoe deformity and is absolutely contraindicated.
Clin Rheumatol. 2012 Jul;31(7):1041-5. doi: 10.1007/s10067-012-1966-8. Epub 2012 Mar 20.
A cohort-controlled trial of the addition of customized foot orthotics to standard care in fibromyalgia.
Source
Department of Medicine, 13-103 Clinical Sciences Building, University of Alberta, 11350-83 Avenue, Edmonton, Alberta, Canada T6G 2P4. rferrari@shaw.ca
Abstract
Customized foot orthotics are widely prescribed for patients with chronic, non-specific low back pain and lower limb pain, but there are few trials demonstrating effectiveness, and none for fibromyalgia. A total of 67 consecutive patients presenting with chronic, widespread pain, who met the 1990 American College of Rheumatology criteria for fibromyalgia, were included in the study. A total of 32 subjects were prescribed a spinal exercise therapy program along with analgesics. These subjects formed the Control group. A second group, comprised of 35 subjects, received the same therapy, along with customized foot orthotics (Orthotics group). All subjects completed the Revised Fibromyalgia Impact Questionnaire (FIQR) at the initiation of the study and at 8 weeks follow-up. The number of subjects using any type of prescription analgesic or other medication for chronic pain at baseline and at 8 weeks was also recorded. A total of 30 subjects in the Control group and 33 in the Orthotics group completed the study. All subjects completed the baseline and 8-week FIQR. The two groups were well matched in terms of age (45.3 ± 11.5 years in the Orthotics group vs. 47.2 ± 8.7 years in the cohort Control), medication use, duration of pain (6.5 ± 4.3 years in the Orthotics group vs. 6.2 ± 3.4 years in the cohort Control group), as well as baseline FIQR scores (55.2 ± 11.0 in the Orthotics group vs. 56.3 ± 12.2 in the cohort Control group). At 8 weeks, the Orthotics group had a greater reduction in the FIQR score than the cohort Control group (reduction of 9.9 ± 5.9 vs. 4.3 ± 4.4, respectively), and this was mainly due to changes in the ‘function’ domain of the FIQR (reduction of 19.6 ± 9.4 in the Orthotics group vs. 8.1 ± 4.3 in the cohort Control group). As part of a complex intervention, in a cohort-controlled trial of primary care patients with fibromyalgia, the addition of custom-made foot orthotics to usual care appears to improve functioning in the short term.
J Orthop Res. 2011 Dec;29(12):1910-5. doi: 10.1002/jor.21477. Epub 2011 Jun 8.
The effect of laterally wedged shoes on the loading of the medial knee compartment-in vivo measurements with instrumented knee implants.
Kutzner I, Damm P, Heinlein B, Dymke J, Graichen F, Bergmann G.
Source
Julius Wolff Institute, Charité-Universitätsmedizin Berlin, Augustenburger Platz 1, 13353 Berlin, Germany. ines.kutzner@charite.de
Abstract
A conventional method to unload the medial compartment of patients with gonarthrosis and thus to achieve pain reduction is the use of laterally wedged shoes. Our aim was to measure in vivo their effect on medial compartment loads using instrumented knee implants. Medial tibio-femoral contact forces were measured in six subjects with instrumented knee implants during walking with the following shoes: without wedge, with 5 and 10 mm wedges under the lateral sole, and with a laterally wedged insole (5 mm). Measurements were repeated with the shoes in combination with an ankle-stabilizing orthosis. Without orthosis, peak medial forces were reduced by only 1-4% on average. With orthosis, the average reduction was 2-7%. Highest reductions were generally observed with the 10 mm wedge, followed by the 5 mm wedge, and the 5 mm insole. Individual force reductions reached up to 15%. Medial force reductions while walking with wedged shoes were generally small. Due to high inter-individual differences, it seems that some patients might benefit from lateral wedges, whereas others might not. Further analyses of the individual kinematics will show which factors are most decisive for the reduction of medial compartment load.
Clin Rehabil. 2011 Apr;25(4):360-9. doi: 10.1177/0269215510386125. Epub 2010 Dec 9.
Efficacy of an insole shoe wedge and augmented pressure sensor for gait training in individuals with stroke: a randomized controlled trial.
Sungkarat S, Fisher BE, Kovindha A.
Source
Department of Physical Therapy, Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai, Thailand. onlaor@chiangmai.ac.th
Abstract
OBJECTIVE:
To determine whether external feedback to promote symmetrical weight distribution during standing and walking would improve gait performance and balance in people with stroke.
DESIGN:
Randomized, controlled, assessor-blinded trial.
SETTING:
Rehabilitation unit and physical therapy department.
SUBJECTS:
Thirty-five individuals with stroke (mean (SD) age = 53.0 (9.3) years) were randomly assigned to an experimental (n = 17) or control group (n = 18). Time post stroke was less than six months for most subjects (n = 27, 77%).
INTERVENTIONS:
Subjects participated in 15 rehabilitation sessions including 30 minutes of gait retraining per session. During gait retraining, the experimental group used an insole shoe wedge and sensors set-up (I-ShoWS) while the control group received a conventional programme. The I-ShoWS set-up consisted of a wedge insole and a footswitch for the non-paretic leg and a pressure sensor on the paretic leg.
OUTCOME MEASURES:
Gait speed, step length and single support time asymmetry ratio, balance and amount of load on paretic leg during stance were evaluated twice: one day before and after training.
RESULTS:
The experimental group demonstrated significant increase in standing and gait symmetry compared with the control group (P < 0.05). They demonstrated 3 times greater improvement in gait speed than the control group (P = 0.02). Balance improvement was significantly greater for the experimental than for the control group (P < 0.05).
CONCLUSION:
Gait retraining using the I-ShoWS set-up was more effective in restoration of gait speed, standing and walking symmetry and balance than a conventional treatment programme. These results indicate the benefit of implementing feedback during gait retraining.
Scand J Med Sci Sports. 2011 Dec;21(6):e42-7. doi: 10.1111/j.1600-0838.2010.01140.x. Epub 2010 Jul 29.
Sever’s injury; treat it with a heel cup: a randomized, crossover study with two insole alternatives.
Perhamre S, Lundin F, Norlin R, Klässbo M.
Source
Centre of Sports Medicine in Värmland, Karlstad, Sweden.
Abstract
Sever’s injury (apophysitis calcanei) is considered to be the dominant cause of heel pain among children. Common advice is to reduce physical activity. However, our previous study showed that application of insoles reduced pain in Sever’s injury without having to reduce physical activity. The purpose of this study was to test which of the two insoles, the heel wedge or the heel cup, provided best pain relief during sport activity in boys with Sever’s injury (n=51). There was a crossover design in the first randomized part of the study. In the second part, the boys, 9-14 years, chose which insole they preferred. There was a reduction in odds score for pain to a fifth (a reduction of 80%) for the cup compared with the wedge (P<0.001). When an active choice was made, the heel cup was preferred by >75% of the boys. All boys maintained their high level of physical activity throughout. At 1-year follow-up, 22 boys still used an insole and 19 of them reported its effect on pain as excellent or good (n=41).
Disabil Rehabil. 2010;32(9):755-64.
The effect of a training program combined with augmented afferent feedback from the feet using shoe insoles on gait performance and muscle power in older adults: a randomised controlled trial.
Hartmann A, Murer K, de Bie RA, de Bruin ED.
Source
Institute of Human Movement Sciences and Sport, ETH, Zurich, Switzerland. antonia.hartmann@move.biol.ethz.ch
Abstract
BACKGROUND:
Aged-related loss of afferent feedback of the feet plays an important role in gait performance. Although strength, balance and gait training can significantly improve the muscle power and functional abilities of older individuals, it remains unclear whether training effects can be enhanced by augmenting afferent feedback from the feet adding shoe insoles complementary to conventional training.
OBJECTIVE:
The current study investigated the effect of physical exercise combined with wearing MedReflex shoe insoles on the gait performance and muscle power in older adults.
METHODS:
Twenty-eight independent living, older adults aged 65-91 years were randomly assigned to either an insole group (IG; n=14) or a training group (TG; n=14). Further 14 subjects matched to the IG and TG were recruited as a control group (CG; n=14) (no exercise). The IG and TG completed the same training program consisting of aerobic exercises, progressive resistance strength training and stretching exercises twice per week for 12 weeks, whereas, the IG wore the insoles during everyday life and during training sessions. Assessments included the Falls Efficacy Scale – International (FES-I), gait analysis and muscle power measurements of the knee and ankle joint at pre- and post-training.
RESULTS:
There were significant time x group interactions in walking speed, step length and in several muscle power measurements. The positive effects of gait parameters ranged between 1% and 12% and between 1% and 8% and the trend to improvements of muscle power ranged between 15-79% and 20-79% for the IG and TG, respectively. The IG and TG did not differ significantly in their improvements. The CG showed a trend to deteriorations between 0% and-5% for gait parameters and between-4% and-14% for muscle power. No significant change in FES-I score occurred in neither groups.
CONCLUSIONS:
The results of this study provide evidence of significant improvements in gait performance and muscle power after a conventional training program in independent living, older adults. However, there is no additional effect of long-term adaptation of gait caused by wearing insoles concurrent to physical training.
Gait Posture. 2009 Feb;29(2):208-13. doi: 10.1016/j.gaitpost.2008.08.007. Epub 2008 Sep 27.
Addition of an arch support improves the biomechanical effect of a laterally wedged insole.
Nakajima K, Kakihana W, Nakagawa T, Mitomi H, Hikita A, Suzuki R, Akai M, Iwaya T, Nakamura K, Fukui N.
Source
Department of Orthopaedic Surgery, University of Tokyo, Bunkyo-ku, Tokyo, Japan.
Abstract
In order to examine if the addition of an arch support could improve the biomechanical effect of the laterally wedged insole, three-dimensional gait analysis was performed on 20 healthy volunteers. Kinetic and kinematic parameters at the knee and subtalar joints were compared among the following four types of insoles; a 5-mm thick flat insole, a flat insole with an arch support (AS), a 6 degrees inclined laterally wedged insole (LW), and a laterally wedged insole with an arch support (LWAS). The knee adduction moment averaged for the entire stance phase was reduced by the use of LW and LWAS by 7.7% and 13.3%, respectively, from that with FLAT. The difference in knee adduction moment between LW and LWAS was most obvious in the late stance, which was ascribed to the difference in the progression angle between those insoles. The analyses also revealed that LW tended to increase step width, and that such an increase was completely eliminated by the addition of an arch support to LW. This reduction of step width could be another mechanism for the further reduction of the moment with LWAS. The analyses of biomechanical parameters at the subtalar joints suggested that LWAS allowed the subject to walk in a more natural manner, while exerting greater biomechanical effects than LW. Thus, the addition of an arch support to the laterally wedged insole reduced knee adduction moment more efficiently, possibly through the elimination of potential negative effects of the laterally wedged insole.
Cranio. 2006 Jan;24(1):50-9.
Immediate effects of plantar inputs on the upper half muscles and upright posture: a preliminary study.
Ciuffolo F, Ferritto AL, Muratore F, Tecco S, Testa M, D’Attilio M, Festa F.
Source
Department of Orthodontics and Gnathology, School of Dentistry, University of Chieti, Italy. fciuffolo.alf@virgilio.it
Abstract
This purpose of this study was to investigate the immediate effects of plantar inputs on both the upper half muscle activity (anterior temporal, masseter, digastric, sternocleidomastoid, upper and lower trapezius, cervical) and the body posture, by means of electromyography (EMG) and vertical force platform, respectively. Twenty four (24) healthy adults, between the ages of 24 and 31 years (25.3 +/- 1.9), with no history of craniomandibular disorder or systemic musculoskeletal dysfunction, were randomly divided into two groups: test group (fourteen subjects) and control group (ten subjects). A first recording session (TO) measured the baseline EMG and postural patterns of both groups. After this session, the test group wore test shoes with insoles that stimulated the plantar surfaces, while the control group wore placebo shoes. After one hour, a second set of measurements (T1) were performed. Significant differences between the groups at baseline were observed in the left anterior temporal, left cervical, and left upper trapezius, as well as at T1 in the left anterior temporal and right upper trapezius (p < 0.05). Within-test group analysis showed a significant increase of the right upper trapezius activity (p < 0.05), whereas no changes were found by within-control group analysis. Lower risk of asymmetric muscle patterns and postural blindness in the test group compared to the control group was observed. Further studies are warranted to investigate the short and long-term effects of this type of insole, in patients with both craniomandibular-cervical and lower extremity disorders.
Clin Biomech (Bristol, Avon). 2004 Nov;19(9):972-7.
The effect of simple insoles on three-dimensional foot motion during normal walking.
Branthwaite HR, Payton CJ, Chockalingam N.
Source
Pennine Acute NHS Trust, Rochdale, Oldham OL12 9QB, UK.
Abstract
BACKGROUND:
The purpose of this study was to establish the effect of simple non moulded flat based insoles on three-dimensional foot motionduring normal walking. Excessive foot pronation is considered a major contributing factor to lower limb injuries. Moulded foot orthoses have been shown to decrease maximum foot eversion. Simple insoles are widely used in clinical practice as an alternative to moulded orthoses. However, there has been little research into the kinematic effects of simple insoles.
METHODS:
All subjects had an inverted rearfoot and forefoot position when the subtalar joint was placed in neutral, which was assessed by a weight bearing goniometer. Rotations of the whole foot about three orthogonal axes relative to the shank were estimated using a five camera motion analysis system.
FINDINGS:
Biplanar insoles significantly (P < 0.05) reduced maximum eversion by an average of 3.1 degrees when compared to the no insole condition. The cobra insole reduced maximum eversion by an average of 2.1 degrees when compared to the no insole condition. This difference approached statistical significance (P = 0.058).
INTERPRETATION:
Biplanar and cobra insoles had no significant effect on maximum dorsiflexion, abduction or rate of eversion, when compared to the no insole condition. These results provide some limited support for the use of simple insoles to control for excessive foot pronation during walking.
Clin Biomech (Bristol, Avon). 2003 Jan;18(1):50-9.
Determination of the effectiveness of materials in attenuating high frequency shock during gait using filterbank analysis.
Source
Department of Human Biology and Nutritional Sciences, University of Guelph, Ont., N1G 2W1, Guelph, Canada.
Abstract
OBJECTIVE:
To develop an accurate method for quantifying the frequency content of the ground reaction force transient.
DESIGN:
Repeated measures design comparing the impact severity during walking with different insole materials.
BACKGROUND:
The body experiences a brief but sizeable impact upon heel strike during walking. This impact transient is believed to result in musculoskeletal injuries. It is important to accurately quantify this impact as a step towards decreasing the risk of injury.
METHODS:
Seven subjects walked barefoot at their normal cadence across a force platform, while insole materials (Spenco, Microcel-puff, and Plastazote) were placed on the surface of the force platform. A filterbank program was developed to determine the percent root mean square in 10 Hz frequency bands from zero to 400 Hz. Analysis focused on the impact transient contained in a 20 ms window after heel contact.
RESULTS:
The high frequency (>60 Hz) power was significantly larger in the barefoot condition compared to the insole conditions. The barefoot condition also resulted in significantly higher initial peak forces and force loading rates.
CONCLUSIONS:
The frequency content of the ground reaction force can be effectively quantified using a filterbank approach. Shoe insole materials can reduce the initial peak force, force loading rate, and frequency content of the impact transient in walking. The frequency content of the initial ground reaction force extends up to 400 Hz in some footwear conditions.
RELEVANCE:
The new filterbank procedure illustrates that the vertical ground reaction force in walking has a higher frequency content than previously thought. This signal requires high sampling rates to avoid aliasing, and appropriate signal processing algorithms, such as filter banks, for analysis.
Int J Sports Med. 2001 Aug;22(6):414-9.
Footwear affects the behavior of low back muscles when jogging.
Ogon M, Aleksiev AR, Spratt KF, Pope MH, Saltzman CL.
Source
Department of Orthopaedic Surgery, University of Innsbruck, Austria. Michael.Ogon@uibk.ac.at
Abstract
Use of modified shoes and insole materials has been widely advocated to treat low back symptoms from running impacts, although considerable uncertainty remains regarding the effects of these devices on the rate of shock transmission to the spine. This study investigated the effects of shoes and insole materials on a) the rate of shock transmission to the spine, b) the temporal response of spinal musculature to impact loading, and c) the time interval between peak lumbar acceleration and peak lumbar muscle response. It was hypothesised that shoes and inserts a) decrease the rate of shock transmission, b) decrease the low back muscle response time, and c) shorten the time interval between peak lumbar acceleration and peak lumbar muscle response. Twelve healthy subjects were tested while jogging barefoot (unshod) or wearing identical athletic shoes (shod). Either no material, semi-rigid (34 Shore A), or soft (9.5 Shore A) insole material covered the force plate in the barefoot conditions and was placed as insolewhen running shod. Ground reaction forces, acceleration at the third lumbar level, and erector spinae myoelectric activity were recorded simultaneously. The rate of shock transmission to the spine was greater (p < 0.0003) unshod (acceleration rate: Means +/- SD 127.35 +/- 87.23 g/s) than shod (49.84 +/- 33.98 g/s). The temporal response of spinal musculature following heel strike was significantly shorter (p < 0.023) unshod (0.038 +/- 0.021 s) than shod (0.047 +/- 0.036 s). The latency between acceleration peak (maximal external force) and muscle response peak (maximal internal force) was significantly (p < 0.021) longer unshod (0.0137 +/- 0.022s) than shod (0.004 +/- 0.040 s). These results suggest that one of the benefits of running shoes and insoles is improved temporal synchronization between potentially destabilizing external forces and stabilizing internal forces around the lumbar spine.
J Bone Joint Surg Br. 2000 Jul;82(5):724-7.
Effectiveness of an insole with a lateral wedge for idiopathic osteonecrosis of the knee.
Uchio Y, Ochi M, Adachi N, Shu N.
Source
Department of Orthopaedics, Shimane Medical University, Shimane-ken, Japan.
Abstract
For the purpose of investigating the effect of an insole with a lateral wedge, we studied 30 patients (31 knees) aged from 46 to 78 years with idiopathicosteonecrosis of the knee for at least three years. The 18 knees treated with an insole (group I) were matched by age, gender, obesity index, area of lesion, femorotibial angle, stage, and clinical evaluation with 13 treated conservatively without an insole (group II). The clinical results, as rated by aknee score, improved significantly more in group I than in group II. Radiologically, the necrotic area and ratio decreased in group I, whereas in group II they increased. In advanced cases, with stage 4 or a femorotibial angle of more than 180 degrees, the use of an insole did not improve the clinical or radiological findings. The insole is a valuable method of conservative treatment for the early stages of osteonecrosis of the medial femoral condyle
Prosthet Orthot Int. 1998 Apr;22(1):35-44.
Primary metatarsalgia: the influence of a custom moulded insole and a rockerbar on plantar pressure.
Postema K, Burm PE, Zande ME, Limbeek Jv.
Source
Sint Maartenskliniek Research BV, Nijmegen, The Netherlands. kp_aro@universal.nl
Abstract
The effects of a custom moulded insole and a rockerbar on peak pressure and force impulse as well as on pain scores in subjects with a history of metatarsalgia were studied. In addition the subjects’ preference for the type of intervention was determined. Forty-two subjects with a history of primary metatarsalgia were selected. They were all provided with the same brand of extra depth shoes with a ready made insole. The effect of custom moulded insoles, a rockerbar and the interaction between the two interventions were studied by testing the four possible combinations: ready made insole without a rockerbar, ready made insole with a rockerbar, custom moulded insole without a rockerbar and custom moulded insole with rockerbar. At the most important region, the central distal forefoot, a rockerbar caused a decrease in force impulse of 15.1% and a decrease in peakpressure of 15.7%. The custom moulded insole produced a decrease of 10.1% in force impulse and of 18.2% in peak pressure. Pain scores were significantly lower for interventions with a custom moulded insole, while the rockerbar showed no influence on pain scores. Subjects with pain preferred a custom moulded insole more often than subjects without pain. Decrease of peak pressure or force impulse was not correlated to pain scores. The use of either a custom moulded insole or a rockerbar produced an important decrease of peak pressure and force impulse at the central distal forefoot and, therefore, either is suitable in any situation which a decrease of pressure is vital.
J Am Podiatr Med Assoc. 1997 Jan;87(1):6-10.
Comparison of Viscoped and PORON for painful submetatarsal hyperkeratotic lesions.
Caselli MA, Levitz SJ, Clark N, Lazarus S, Velez Z, Venegas L.
Source
Department of Orthopedic Sciences, New York College of Podiatric Medicine, New York, USA.
Abstract
A clinical study was performed to evaluate the efficacy of the Viscoped Insole as compared with an 1/8-inch PORON medical materials insole in the treatment of lesser submetatarsal hyperkeratotic callosities. Thirty-five patients, ranging in age from 23 through 61 years (average 42 years) were randomly divided into three groups. All three groups initially had debridement of their submetatarsal callosities. In addition to the debridement, the first group (16 patients) wore a Viscoped Insole for 4 weeks. The patients in the second group wore a PORON insole for 4 weeks. The third group did not receive an insole after their debridement and served as the control. There was a significant improvement in the Viscoped group and the PORON group versus the control group (x2 = 40; p < 0.01) as measured by the foot function index. Insole therapy combined with debridement for submetatarsalhyperkeratoses is more effective than debridement alone.
Lepr Rev. 1996 Sep;67(3):208-16.
Cost-effective footwear for leprosy control programmes: a study in rural Ethiopia.
Abstract
A randomized, controlled trial of commercially available canvas shoes was carried out in a rural area of Ethiopia. Subjects with deformed and anaesthetic feet, most with ulceration, were given either canvas shoes or plastazote/moulded shoes and followed up for one year. Seventy-five percent of subjects with ulcers who used canvas shoes had no ulcer at the end of the study, while no significant change was noted in the plastazote group. The durability and acceptability of the shoes were also examined. Clients in remote areas who have no access to an orthopaedic workshop, but who have anaesthetic feet, with or without deformity, should have access to canvas shoes with an MCR insole. Two pairs are needed per year at a cost of US$6.7 per pair.
J Am Podiatr Med Assoc. 2004 May-Jun;94(3):239-45.
Plantar pressures in rheumatoid arthritis using prefabricated metatarsal padding.
Jackson L, Binning J, Potter J.
Source
Southampton City PCT, Podiatry Services, Central Health Clinic, Southampton, England.
Abstract
We sought to determine whether one of two prefabricated insole designs could better manage high forefoot plantar pressures in patients with rheumatoid arthritis. Ten subjects with rheumatoid arthritis who experienced pain with shod weightbearing were studied by using a plantar pressuremeasurement system. Two insole designs and a shoe-only control condition were randomly tested in repeated trials. Dome- and bar-shaped metatarsal pads made of latex foam were incorporated into full-length insoles made of urethane. Significant reductions in mean peak plantar pressures over the central metatarsals were noted when using the insole and dome pad design (12% [33 kPa]) and the insole and bar pad design (21% [58 kPa]) compared with the shoe-only condition. A prefabricated insole design incorporating a bar metatarsal pad is recommended to manage high forefoot plantar pressures in patients with rheumatoid arthritis.
